


Background and Significance
According the Thai Elderly report published in 2015, Thailand has a population of 10.3 million people aged 60 and older, accounting for 16% of the total population. It is the second highest percentage of elderly people in ASEAN countries. According to the United Nations’ definition, a country that has a population of people over 60 years old accounting for more than 10% of its total population is officially becoming an aging society; and it would completely become an aged society when this proportion has increased to 20% of the total population. Thailand is likely to become the highest aging society in 10 years. The Office of National Economic and Social Development Board has estimated that the population of Thais aged 60 and older will be over 20% by 2021 and will be the age group with the largest percentage of the population (28%) in 2031 (Prasartkul, 2016).
According to the population survey of the 2016 fiscal year by the Lampang Provincial Health Office, Lampang has a total population of 573,247. The number of the people aged 60 and older is 142,932 (24.93% of the total population). Lampang has a high percentage of the population aged 60 and over, which is higher than the overall percentage of the country. The five districts with the highest percentage of the population aged 60 and older are (1) Mae Phrik, 33%, (2) Sop Prap, 30.40%, (3) Thoen, 28.02%, (4) Mae Tha, 27.72%, and (5) Kho Kha, 27.06%.
In Mae Tha, there are 10 sub-districts with a total population of 48,786. Among them, there are 13,487 people or 27.72% of the total population aged 60 and older. After asking about Activities of Daily Living (ADL), the results showed that 95.20% of the elderly were in a group of social-bound (ADL scores ≥ 12), 4.20% were in homebound (ADL scores = 5-11), and 0.60% was bedridden (ADL scores = 0-4). The health report of the elderly found several diseases, which included osteoarthritis (22.45%), oral disorders (14.73%), cataracts (8.73%), dementia (4.28%), and depression (1.46%) (Mae Tha Hospital, 2016).
The Nam Cho Sub-district in Mae Tha, Lampang, was selected as a provincial prototype for long-term care of the elderly people. There are 2 health promotion hospitals in Nam Cho Sub-district, namely Hong Ha and Ban Nong. With the population of 3,182 people in Hong Ha community 27% aged 60 and over; and with the population of 4,870 people in Ban Nong community, 24.64% aged 60 and over. Both hospitals, Hong Ha Health Promoting Hospital and Ban Nong Health Promoting Hospital, are health-promotion institutions with a complete care for “The Elderly Society” (more than 20% of the total population over 60 years old). The researcher has selected the study area of Hong Ha Health Promoting Hospital due to the high percentage of the population aged 60 and older cared for there. The community is likely to become a “Super Aged Society” (more than 28% of the total population over 60 years old) (Lampang Provincial Health Office, 2016).
Hong Ha Health Promoting Hospital (Hong Ha HPH) is responsible for 3,182 people from Villages 1, 6, 7 and 8 of Nam Cho District, including 859 people age 60 and older. After classification by the Barthel Index of ADL, the results showed that 797 were social- bound (79.78%), 50 were homebound (5.82%), and 12 were bedridden (1.40%). Over time, some of the social-bound elderly have become dependent. From the preliminary survey, it has been found that some dependent elderly people do not have family caregivers to care for them. In this case, a volunteer takes over. The results also revealed that elderly people are at a high risk of developing complications like ankylosis, pneumonia, bedsores, urinary tract infections, falls, and mental health problems such as feelings of worthlessness, depression, and aggressiveness. It was reported that caregivers who take care of dependent elderly people feel stressed by long-term care and there are chances of family economic problems.
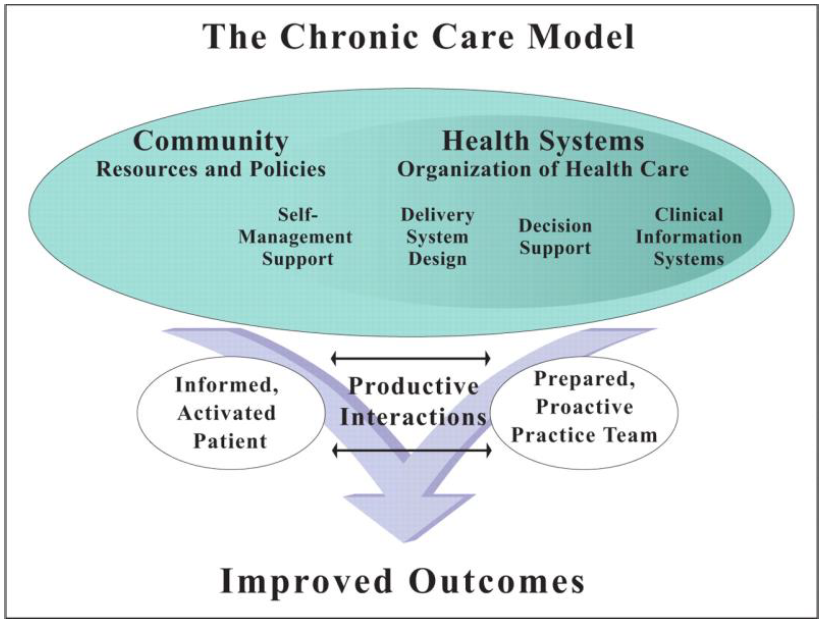
Based on the information and conditions of the problems, the researcher was interested in studying the health status of dependent elderly people and characteristics of caregivers in order to obtain information for appropriate health care services according to the Chronic Care Model, which consists of six components: self-management support, delivery system design, decision support, clinical information system, health systems organization, and community resource linkages. These key components would enable elderly people and caregivers to have a good quality of life and live in the community with dignity.
Objectives
-
To study the health status of dependent elderly people.
-
To study the behaviors of caregivers.
-
To describe the caring components for dependent elderly people.
The researcher applied the Chronic Care Model to describe the caring system for dependent elderly people in the community. It consists of 6 connected elements as shown in Figure 1.
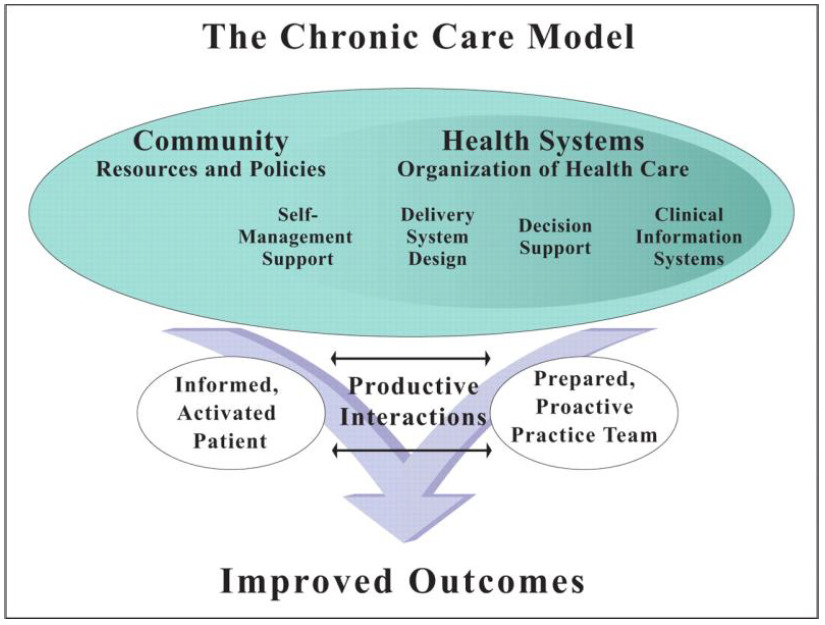
The six components of the Chronic Care Model are as follows:
1. Self-management support is to create recognition of self-reliance in health care among the elderly people and caregivers.
2. Delivery system design is the design of the service system from three main community partners involving three principles, which are a team-based approach, planned care visits, and case management.
3. Decision support is the way to support three main partners in the community to apply useful and up-to-date knowledge in operating help systems to make further decisions in health care service (e.g., expert advice and transfer system).
4. Clinical information system is the knowledge system related to useful elderly health care information for focusing on further improvement.
5. Health systems organization is aimed to promote leadership, vision, and mission or project planning regarding the elderly health care services of the three main partners.
6. Community resource linkages are the sharing of resources between the three main community partners to achieve effective long-term care.
Dependent elderly people experience health problems caused by age-related deterioration or complications from previous illnesses or current illness, and for this reason, they need health care from families, communities, and government sectors or private organizations. The assessment of physical, mental, and social health of the elderly people in Phetchabun Municipality found that some elderly people were grouped either homebound or bedridden (Ngoichansri & Kongtaln, 2012). Both groups experienced certain health problems such as: (1) Physical health problems: excessive body mass index, diseases (high blood pressure, diabetes, high blood lipids), tooth decay or caries/gum disease/no teeth, which later cause trouble in chewing food, deafness or reduced hearing, bone and muscle pain (lumbar pain, back pain, joint pain), defecation problems (constipation) and urinary excretion problems (urinary incontinence and leakage); (2) Mental health problems: depression, lack of self-reliance, family problems and concerns, and (3) Social health problems: inability to participate in social activities.
Wirojratana, Amnatsatsue, Sasat, Malathum, and Narongsak (2014) developed a model of health care service for dependent elderly people by engaging family, community, and government organizations through participatory action research. The research has concluded that caregiving for dependent elderly people should include three main components: caregiver and family, community network, and health care service center. Each component is supported and coordinated in the care of elderly by integrating health and social services. The experiment was conducted in three communities and the result showed an increasing number of elderly who accessed services, along with higher service satisfaction.
The use of a participatory model in conducting research has led to a better understanding of social integration of all components in having mutual learning and caring. It empowers older people and their families to be connected with the community, and this leads to the formation of a horizontal relationship. In addition, there is qualitative research that discusses community networks involving care for dependent elderly people in the northeast of Thailand (Sawatphol et al., 2017).
The purpose of this research was to study an appropriate way to care for elderly people in the northeastern region of Thailand. The results of this research concluded that there are two systems in the health care of dependent elderly people. The first one is “home care” where the dependent elderly people receive health care from family members who take care of their health, provide economic support, and take care of their daily living needs. The second one is “community care” where dependent elderly people receive health care from relatives, neighbors, village leaders or directors, organized volunteers, or groups in local communities (e.g. Village Health Volunteers,Social Development and Human Security Volunteers, community caregivers, monks, and members of Community Elderly Club, local government staff and government officers).
Research Methodology
This research used a descriptive method to conduct a survey and structured interviews on the health status of dependent elderly people and characteristics of caregivers to obtain information on the provision of health service provided to elderly people.
Sample Population
The sample used in this study were dependent elderly people and primary caregivers, known as family members or relatives of the dependent elderly people, from four villages within the responsibility of Hong Ha Health Promoting Hospital in Nam Cho Sub-district (Village 1, Village 6, Village 7, and Village 8). The researcher selected the sample by purposeful sampling.
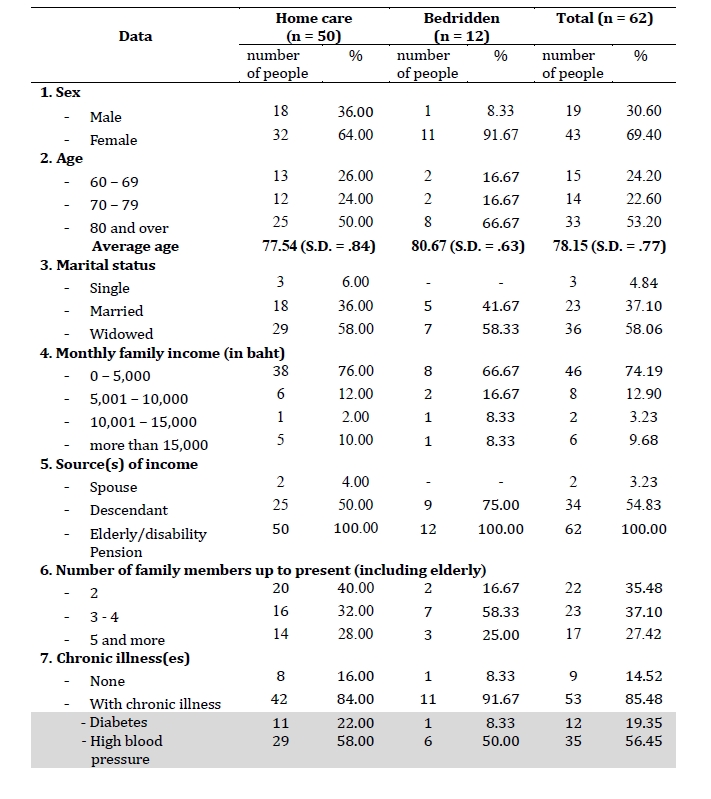
The first group consisted of 62 dependent elderly people from Village 1, Village 6, Village 7, and Village 8 who received an assessment on their ability to perform activities of daily living using the Barthel Index of ADL, in which the scores ranged from 0-11/20. The second group consisted of the 62 primary caregivers of these elderly people.
The group of 62 dependent elderly people consisted of 50 home care elderly people (ADL scores = 5-11) and 12 bedridden elderly people (ADL scores = 0-4).
.jpg)
Research Tools
Research tools consisted of:
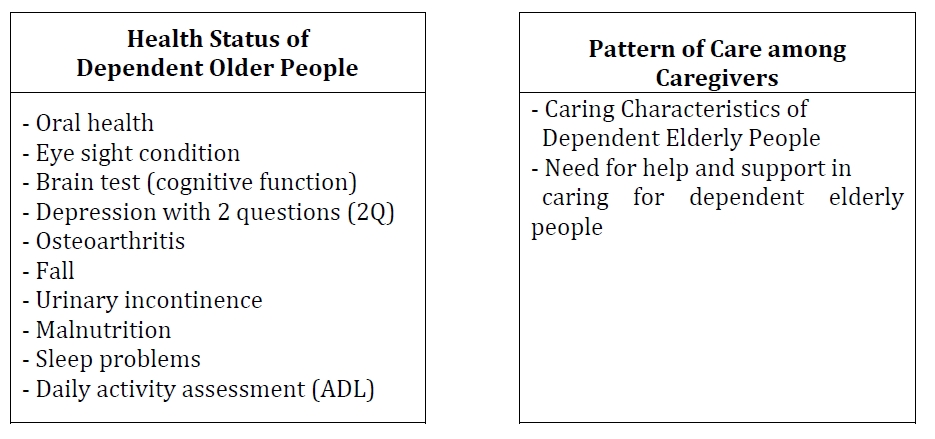
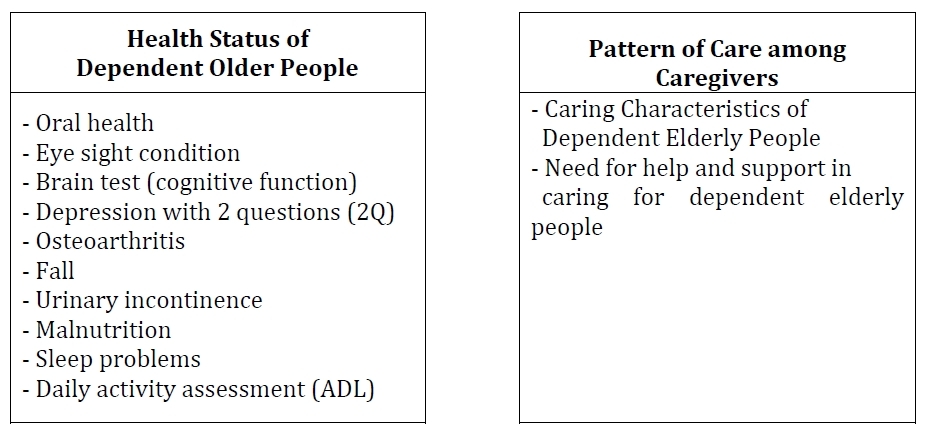
1. Elderly Health Status Screening and Assessment (Department of Medical Services, Ministry of Public Health, 2015) associated with oral health, eyesight condition, brain test (cognitive function), depression assessed with 2 questions (2Q), osteoarthritis, falls, urinary incontinence, malnutrition, sleep problems, and daily activity assessment (ADL).
2. Structured interviews consisted of open-ended questions on dependent elderly care and the need for support in caring.
Data Collection Period
The researcher collected the quantitative and qualitative data collection from February to July 2017.
Data Analysis
1. General information, screening data, and health status assessment were analyzed using frequency, percentage, mean, and standard deviation.
2. From the interview data of dependent elderlyand caregivers, the researcher examined the validity of the data, organized data and keywords summarized in two topics, “Caring Characteristics of Dependent Elderly People” and “Need for help and support in caring for dependent elderly people.”
Results
The data analysis has been divided into three parts as follows: 1) General data and data from screening and assessment of dependent elderly health status, 2) General information and data on health care for dependent elderly (home care and bedridden) from caregivers, and 3) Interview information from caregivers in health care (home care and bedridden) and the need for supportive care.
Part 1: General Information and Data from Screening and Assessment of Dependent Elderly Health Status

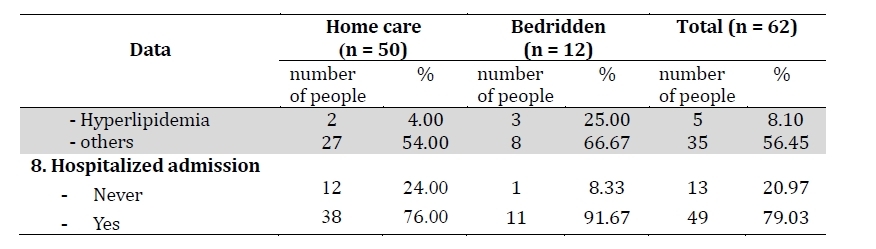
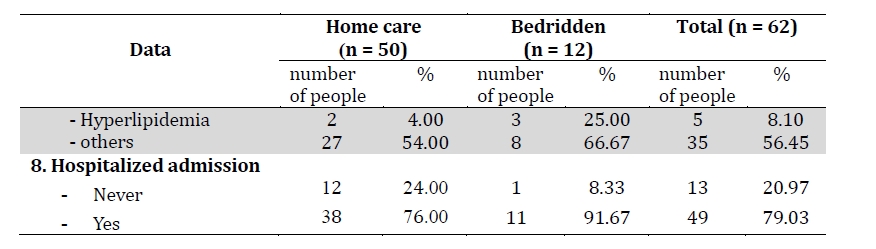
As shown in Table 2, the majority of dependent elderly were female (69.40%) with an average age of 78.15 years. The age of the bedridden elderly group was significantly higher than home care (80.67 and 77.54 respectively). Most were widowed (58.06%) and the average family monthly income was less than 5,000 baht (approximately $155 US; 74.19%) from elderly/disability pension. Of the 62 elderly people, 85.48% of them had diseases such as diabetes, high blood pressure, hyperlipidemia or high blood lipid levels, and 79.03% of them had been admitted to the hospital in the past 5 years.

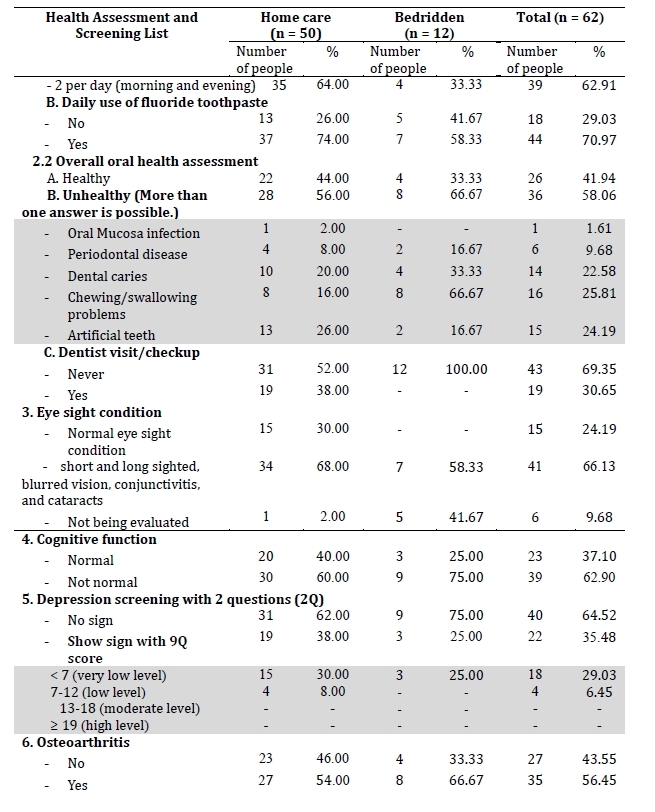
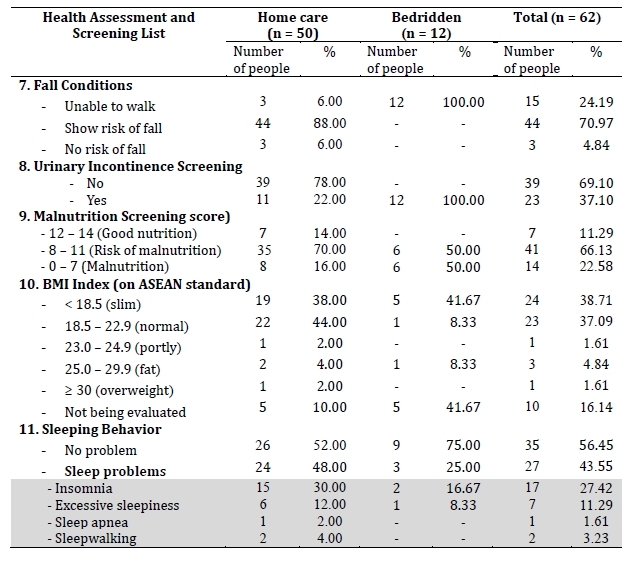
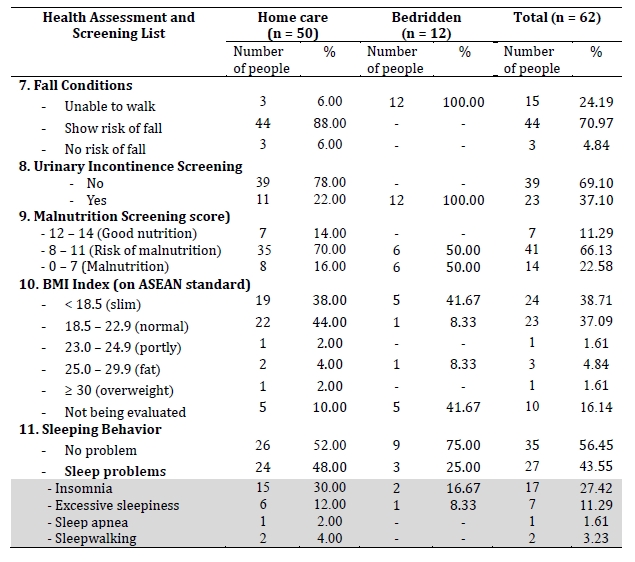
Table 3 shows that the majority of dependent elderly people in the home care group had an ADL score of 11 (78%), and the majority in the bedridden elderly group had an ADL score of 3 (58.34%). According to an oral health assessment, although the majority of dependent elderly patients brushed their teeth twice a day, 58.06%, had oral health disorders such as oral mucosa infection, periodontal disease, dental caries, chewing and food swallowing problems, and/or the use of artificial teeth. Of the 62 elderly people, 66.13% had eye problems, such as being near- or far-sighted, and/or having blurred vision, conjunctivitis, and/or cataracts. Most of them had knee pain and were at risk for falling (70.97%) and risk of malnutrition (66.13%). Some elderly people had BMI below the standard of ASEAN (38.71%). Some had urinary problem or incontinence (30.65%). There were 35.48% who suffered from depression based on a 2-question scale, and 43.55% had trouble sleeping, such as, insomnia, excessive sleepiness, sleep apnea, and sleepwalking.
Part 2: General Information and Data on Health Care for Dependent Elderly (Home Care and Bedridden) of Caregivers
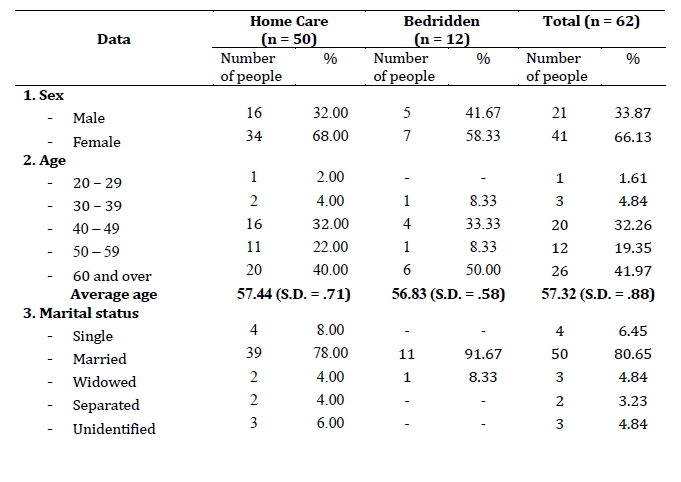
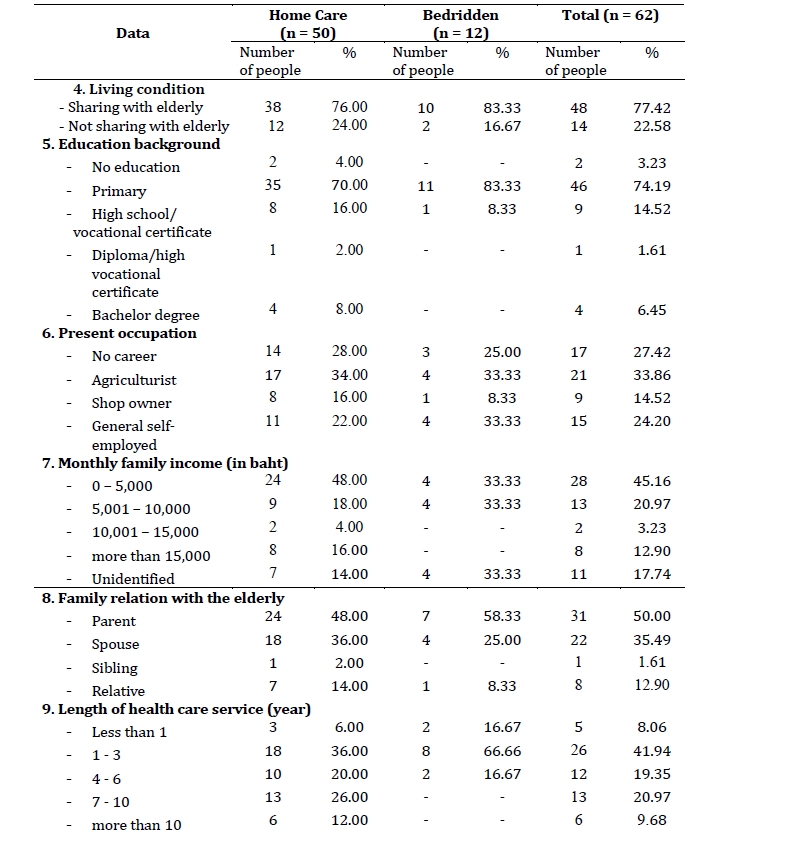
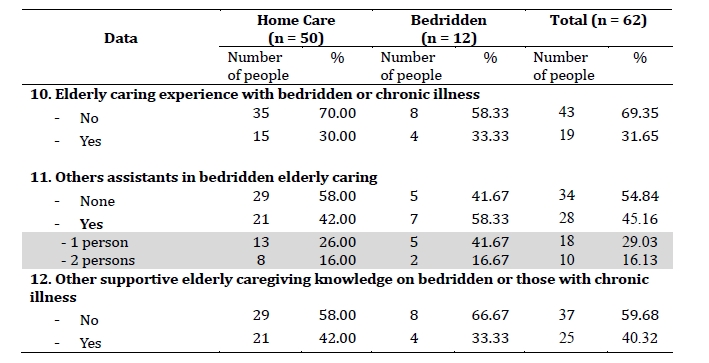
According to Table 4, most of caregivers were female (66.13%) with an average age of 57.32 and married (80.65%). The percentage of those sharing a house with dependent elderly was 77.42%. As for their educational background, the majority of caregivers had a primary school education (74.19%). Most of them were farmers (33.86%) with an average monthly income of less than 5,000 baht (45.16%). It was commonly found that the elderly person was the parent of the caregiver. The most common length of care giving was 1-3 years (41.94%), and most of them had no professional experience in elderly caregiving (69.35%). Some caregivers were assisted by others in caring for the dependent elderly (45.16%), and most of them had not received any knowledge regarding caring for the elderly, the injured or chronic conditions (59.68%).
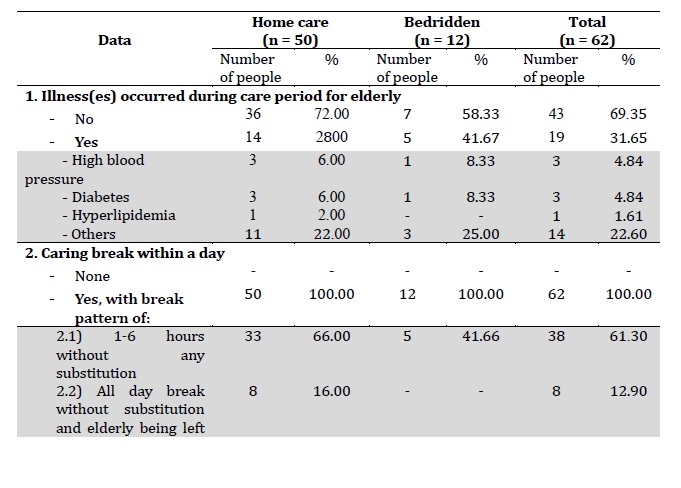
.jpg)
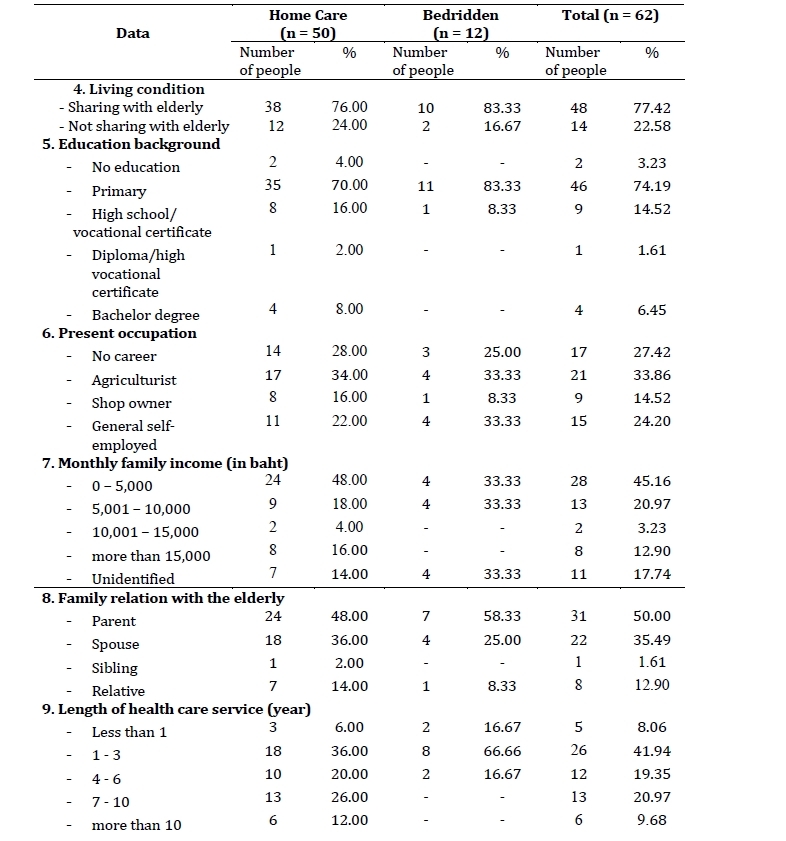
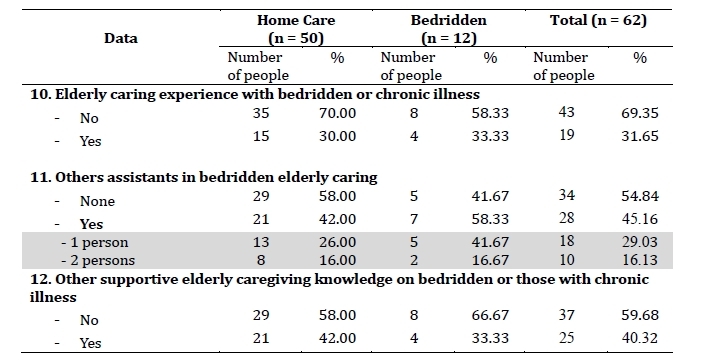
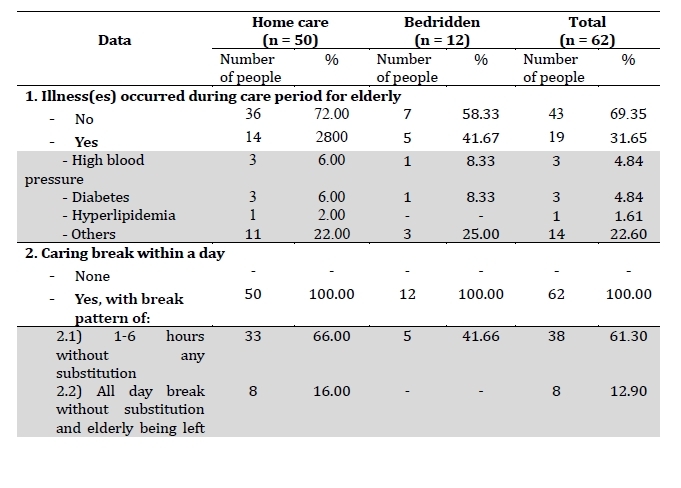
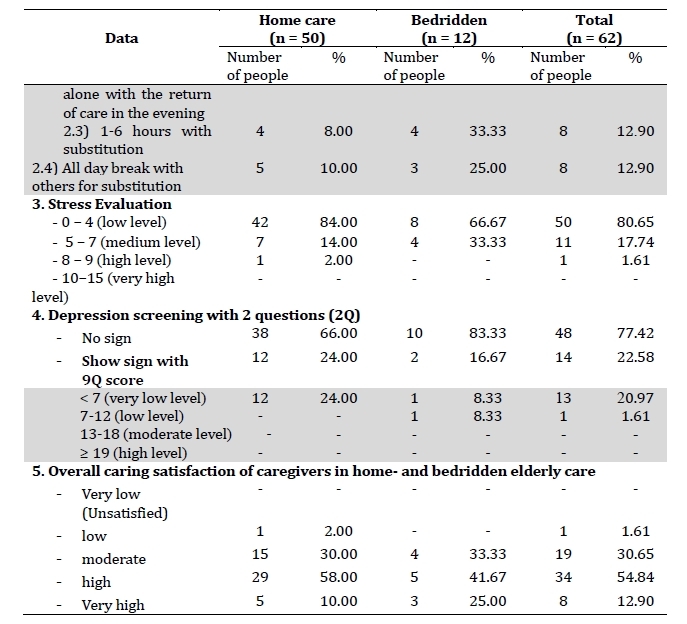
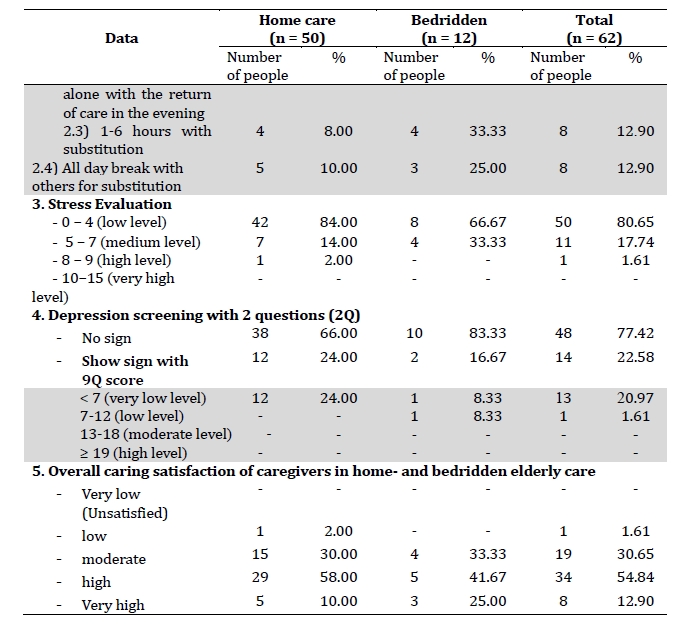
Table 5 shows the percentage (31.65%) of caregivers who experienced illnesses while caring for a dependent elderly person. Diseases or illnesses found were diabetes and high blood pressure. Caring breaks during the day varied from 1-6 hours through all day. A majority (61.30%) of the elderly were found to be left alone while caregivers were on a break. Some (12.90%) of the caregivers left the homebound elderly person during the day and returned in the evening. The majority of caregivers were found to have small amount of stress, while 77.42% had no depression. Most caregivers had an overall satisfaction toward caregiving at a high level (54.84%), followed by a moderate level (30.65%).
Part 3: Information on Pattern of Care among Caregivers Caring Characteristics of Dependent Elderly People:
Cleanliness. Most of the dependent elderly people took a bath twice a day. Independent elderly people were provided with washing facilities by the caregiver, such as bath accessories, clothes, and diapers. The independent elderly people would clean their body, change clothes, and diapers by themselves. Those with difficulties in taking a bath or who had limited mobility, were assisted by caregivers. Bedridden elderly people were fully assisted by caregivers in taking a bath or cleansing their body. In some cases, it was necessary to change the method of cleaning the body from giving a bath to giving a sponge bath instead.
Health Care. Most caregivers provided timely assistance to the elderly people, including food preparation and administering medicines. Risk of fall prevention was also provided by caregivers in the homes of the elderly people with diminished mobility. The caregivers were also responsible for taking the elderly people to the hospital for checkups, and for providing medication, including insulin injections for those with diabetes.
Environmental and Residential Care. Most caregivers cleaned the bedding and clothes of the elderly people. They also cleaned the rooms and the rest of the house. In some instances, fall prevention equipment had been installed by some caregivers.
Mental Health Care. Most caregivers occasionally had a conversation with the elderly people during their daily activities. There were some neighbors who paid a visit and talked to the dependent elderly people whose caregivers went to work. In some cases, elderly people were left alone in their bedrooms, inside their houses, or in the open area on the first floor.
Need for help and support in caring for dependent elderly people
Nam Cho Sub-district Municipality should provide elderly care devices such as walking sticks, canes, beds, diapers, and other supplies. In addition, the government should allocate sufficient budget to support caregiving for the bedridden elderly people and to those with disabilities.
A budget from the government and Nam Cho Sub-district Municipality to encourage family members to work at home or go out to work would be pivotal. Due to the burden of caring for bedridden and dependent elderly people, caregivers should be promoted or rewarded by having a career and earning income.
Frequent visits by doctors, nurses, or village health volunteers are required and important. With their professional skills, they are able to provide advice and proper knowledge to caregivers, including health checkups at home. This is necessary because of the difficulty of moving dependent elderly people to hospitals.
Frequent visits by community leaders, volunteer groups, or staff from Nam Cho Sub- district Municipality could provide support for caregivers and the elderly. It also would benefit the visitors to know more about the health care needs of elderly people, and therefore provide an appropriate quality of care for them.
Overall Results
The results of the research found that among 85.48% of dependent elderly people, 79.03% had diseases such as diabetes, high blood pressure, hyperlipidemia, or had been hospitalized. Of the dependent elderly, 58.06% had oral health disorders such as oral mucosa infection, periodontal disease, dental caries, chewing and food swallowing problems, and the use of artificial teeth. Eyesight problems (66.13%) included both near- and far- sightedness, blurred vision, conjunctivitis, and cataracts. Most of the elderly people (70.97%) had knee pain and were at risk of falling. The percentage of malnutrition risk was 66.13% while some of them (38.71%) had BMI index below the standard of ASEAN. Urinary incontinence and leakage was present in 30.65%. Some (43.55%) experienced sleep problems such as insomnia, excessive sleepiness, sleep apnea, and sleepwalking.
The caring characteristics of dependent elderly people by the caregivers included cleanliness, health care, environmental and residential care, and mental health care. In addition, the need for help and support in caring consisted of elderly care devices, increased funding, and visits by doctors, nurses, or village health volunteers, community leaders, volunteer groups, or staff from Nam Cho Sub-district Municipality.
Discussion
This research used the Chronic Care Model to describe the caring system for dependent elderly people in the community. This model has the following 6 components: 1) Self-management Support, 2) Delivery System Design, 3) Decision Support, 4) Clinical Information System, 5) Health Systems Organization, and 6) Community Resource Linkages.
Dependent elderly people who are able to help themselves through self-care should be motivated and encouraged to continue to do so especially when they have chronic illnesses and take medication or have any other kind of treatment. In addition, they should be encouraged to have a better understanding of their chronic illnesses. Skills of living with chronic illnesses should be added to their knowledge, so that they can evaluate the barriers and the need for further resources to support their care. Moreover, related community agencies should participate in designing a delivery system to care for dependent elderly people. Consequently, proper ways to support decision-making ability and to select appropriate combinations of care, including case management for home care and bedridden dependent elderly people, are very important and can help people achieve better outcomes. Planned care visits should be formed as a team-based approach to cover the needs of caring for elderly people who are physically, emotionally, socially, spiritually, and/or economically dependent. Clinical information systems have been used as an aid in collecting data to serve as a database in regards to planning follow-up care for the dependent elderly people. This will be useful in information sharing among teams or agencies involved in the care of dependent elderly people, as it reflects an effective system for teamwork.
Based on the need for supportive care in dependent elderly people in terms of care equipment, raising elderly people’s pension, promoting careers at home to caregivers, and relocating the elderly to the hospitals, the research found that most caregivers (59.68%) did not receive any knowledge about caring for the elderly people or dependent elderly people with chronic diseases. This reflects health care management on national, provincial, and district levels. Relevant visions, policies, and work plans should be introduced to develop all categories of elderly population. Community resource linkages should be used to integrate community resources in either small or large health care service units such as local government organizations and private sectors (Gomutbutra & Thongbunjob, 2008). Related practices should concern inpatient transfer policies, career and income promoting systems, skills and potential enhancement for caregivers to care for elderly people, elderly value support to family members and relatives, and public stimulation on the importance of caring for older people who are part of the community.
Suggestions
1. Agencies involved in the care of dependent elderly people in the Hong Ha community should work together. Integrated work should begin with establishing visions, policies, and project plans to support elder care activities. Each agency should set clear roles and responsibilities to reduce duplication of work and to coordinate the use of resources together to achieve cost-effectiveness and efficiency.
2. The data from the assessment and screening of the health status of dependent elderly people and caregivers should be included in the care plans of the Hong Ha Health Promoting Hospital. Continuous care in care plans should deal with the different conditions and needs of the dependent elderly people and caregivers.
3. In the Hong Ha community, family members and relatives are still the primary caregivers. It has been shown that family bonds and relationships among family members in Thai society are still strong. Therefore, health care skills and knowledge in caregivers should be developed and promoted to provide care for dependent elderly people according to individual needs. In particular, health care teams should encourage caregivers to increase their potential and confidence in caring for the elderly people. Advice and suggestions should be given to caregivers who care for the elderly with complex health conditions.
4. Social-bound elderly people in Hong Ha community should be supported by the community to help elderly people with dependence. The establishment of volunteer groups, such as “Friends Help Friends,” could provide physical assistance, counseling, and daily use equipment to dependent elderly people.
5. The use of technology to care for the elderly with dependence in the community should be promoted. For example, the use of LINE GROUP for caregivers could allow members of the group to share ideas together, learn about caring, consult about problems, and coordinate with relevant agencies.
Biographical Notes
Sumitra Wicha, M.N.S., is a nursing instructor in the Adult & Aging Nursing Department at Boromarajonani College of Nursing Nakhon Lampang. Her research interests include health promotion in NCD people, long-term care systems in the community, and ethics in clinical practice.
She can be reached at Boromarajonani College of Nursing Nakhon Lampang, 268 Pa-kam Rd., Hua-Wiang, Lampang 52000, Thailand, by telephone at +66-5422-6254 connect 113, by fax at +66-5422-5020, by mobile phone at +66-89-700-3982, or by e-mail at <sumitra18@hotmail.com.>
Benjaporn Saovapha, M.P.A., is a nursing instructor in the Adult & Aging Nursing Department at Boromarajonani College of Nursing Nakhon Lampang. Her research interests include organization development in nursing administration and orthopedic nursing.
She can be reached at Boromarajonani College of Nursing Nakhon Lampang, 268 Pa-kam Rd., Hua-Wiang, Lampang 52000, Thailand, by telephone at +66-5422-6254 connect 113, by fax at +66-5422-5020, by mobile phone at +66-87-466-3453, or by e-mail at <benja8196@hotmail.com.>
Sirirat Sripattarangkul, M.N.S., is a nursing instructor in the Adult & Aging Nursing Department at Boromarajonani College of Nursing Nakhon Lampang. Her research interests include health promotion in NCD people and patient advocacy.
She can be reached at Boromarajonani College of Nursing Nakhon Lampang, 268 Pa-kam Rd., Hua-Wiang, Lampang 52000, Thailand, by telephone at +66-5422-6254 connect 113, by fax at +66-5422-5020, by mobile phone at +66-81-724-2409, or by e-mail at <lek1f@yahoo.co.th.>
Natchapan Manop, M.P.H., is the Director of Public Health and Environment Division in Nam Cho Sub-district Municipality. Her research interests include health promotion in the community.
She can be reached at Nam Cho Sub-district Municipality, 111 village 5, Nam Cho Sub-district, Maetha District, Lampang 52150, Thailand +66-5434-6238, by fax at +66-5434-6238 connect 12 +66-86-587-0962, or by e-mail at <Natchapan.ma@gmail.com.>
Thanakrit Muankonkaew, M.S., is an Instructor at the Public Health Faculty at Nation University. His research interests include food and nutrition for NCD people and epidemiology in the community.
He can be reached at Nation University, 444 Prabat Sub-district, Wattana Rd., Muang, Lampang 52000 Thailand, by telephone at +66-5426-5170 connect 6, by fax at +66-5426- 5184, by mobile phone at +66-86-921-0054, or by e-mail at <chutchai_mua@nation.ac.th.>
Supha Srirungrueang, M.N.S., is the Director of Hong Ha Health Promoting Hospital and is interested in case management in NCD and long-term care patients.
She can be reached at Hong Ha Health Promoting Hospital, 222 Village 1, Nam Cho Sub-district, Maetha District, Lampang 52220, Thailand, by telephone at +66-5434-6326, by mobile phone at +66-88-503-8802 or by e-mail at maetha_06222@hotmail.com.
Date of submission: 2018-03-06
Date of the review results: 2018-03-23
Date of the decision: 2018-04-10