
Introduction
Cancer is a severe chronic disease and is considered to be a major global health problem. At present, cancer is the second cause of death worldwide and the number of new cancer patients continues to increase. The American Cancer Society predicts that in 2030, there will be 21.4 million new cancer patients and rate 13.2 million deaths from cancer worldwide (American Cancer Society, n.d.). In Thailand, cancer is the number one cause of death with 77,566 deaths in 2016 or 119.90 people per 100,000 people (Strategy and Planning Division, 2017).
Cancer is caused by abnormal cell growth resulting in changes in the body. It can sometimes be cured if found in the early stages but cannot usually be cured when it reaches an advanced stage (World Health Organization, 2014). Advanced cancer patients need to be treated with palliative care in order to relieve suffering and improve quality of life. Then they can face death and have a “good death” (Cancer Council Australia, 2016). A good death is based on a pain-free status and following specific preferences for the dying process (Meier et al., 2017). Good death is the outcome of a good preparation for death, including acceptance of death (McLeod-Sordjan, 2014). From prior studies, it was found that few cancer patients accept death. Pinquart et al.‘s (2006) study showed that in their sample (n=337) the mean score of the cancer patients’ death acceptance was 14.9 indicating a moderately low rate of acceptance. Moreover, Hinton (1999) found that 49% of cancer patients (n=76) had a low rate of the death acceptance and 18% failed to accept death and denied death was coming.
Death acceptance means the perception and expression that death is a truth of life that is unavoidable and a lack of fear. Patients who accept death will prepare for it, as well as prepare their family, and plan to face death (Thongdam et al., 2015). Patients who deny death will continue to seek treatment for their healing; furthermore, they may have grievances and blame others for their condition; such as, blaming the delayed hospital system for worsening their disease. In addition, they may fear death, have anxiety, and feel depressed (Visalo, 2009), all of which tend to lead to a more conflicted and uneasy death (Zimmermann, 2012). Alternatively, a good death acceptance results in the patients’ good death (McLeod-Sordjan, 2014; Payne et al., 1996). As such, helping patients come to accept death as something that will happen eventually is a psychosocial support for patients with advanced cancer so that they will be able to face death in peace; thus, nurses can play an important role in helping patients to accept death (Visalo, 2009).
Prior research in Germany and the United States of America (USA) found that impairments in the activities of daily living (ADLs), poor prognosis, no goals in long-term future planning, high religious beliefs, increasing age, high perception of self-efficiency, and less anxiety about death were related to death acceptance in healthy persons, chronically ill patients, and cancer patients receiving chemotherapy for the first time (Daaleman & Dobbs, 2010; Harding et al., 2005; Pinquart et al., 2006). According to this evidence from the Western perspective, different cultures and religious traditions viewed death acceptance differently. In addition, Pinquart et al. (2006) showed that, among cancer patients receiving chemotherapy for the first time, having stronger physical impairments was correlated with higher levels of death acceptance. There is a gap in research about other stages of cancer, such as advanced cancer. In Thailand, 94% of the population is Buddhist (National Statistical Office, 2018), and so the factors predicting death acceptance of advanced cancer patients in the Thai context need to be studied. Therefore, this research aimed to study the factors associated with death acceptance among Thai advanced cancer patients.
Methodology
This quantitative study with a cross-sectional research design explored associative factors for death acceptance of patients with advanced cancer.
Participants
The participants were patients who received palliative treatment from outpatient cancer clinics in three tertiary hospitals in Bangkok, Thailand. The inclusion criteria: who were between 18-59 years old, were Buddhist, and had been diagnosed as stage 3 or 4 cancer patients, and all had palliative care as the treatment goal. The patients were not having complications from their advanced diseases or if they were in grief and/or bargaining stages of acceptance using Kubler-Ross’s (1997) assessment of the five stages of grief. Finally, the participants and their family caregivers had to be willing to participate in the research. The researchers used multi-stage sampling to select the three hospitals and convenience sampling for the participants.
The sample size was determined by the power of test analysis using the G* Power Version 3.1.9.2 program for the F test of the variance explained by the overall regression equation with a model containing 7 independent variables (Faul et al., 2007), which was determined using the power of the test at 95%. This showed a statistical significance of .01 level with at least 151 participants. There were 242 subjects who participated in this research.
Instruments
-
Personal Information Questionnaire. This questionnaire was comprised of information about gender, age, marital status, education level, occupation, type of cancer, stage of cancer, and duration of illness.
-
Death acceptance scale is a neutral acceptance dimension of The Death Attitude Profile Revised by Wong et al. (1994). The researchers translated this instrument into the Thai language by using a back-translation method. It is composed of five items and a 7-point Likert scale, which were strongly agree = 7 to strongly disagree = 1. The score interpretation from the total score ranged between 7-35 points. High scores meant high levels of death acceptance. Cronbach’s alpha of this scale was .70.
-
The Death Anxiety Questionnaire (DAQ) by Conte at al. (1982) was translated into the Thai language by the researchers using a back-translation method. The questionnaire consisted of 15 items covering four dimensions: 1) Fear of the Unknown, 2) Fear of Suffering, 3) Fear of Loneliness, and 4) Fear of Personal Extinction. In each item, there were three rating scales with a score from 0-2; 0 was no anxiety and 2 was the most anxiety. The scores ranged from 0-30 and high scores meant a higher level of death anxiety. Cronbach’s alpha was .86.
-
Buddhist Beliefs about Death Questionnaire developed by Rangsikosai et al. (2013). It was developed based on the Buddhist principles, “Dtrai lak” or “the three characteristics of existence.” It consisted of 13 items. The answers were arranged in three scale levels; namely, strongly belief (3 points) to weak belief (1 point). The total score ranged between13-39; the high score meant a high level of religious belief about death. Cronbach’s alpha was .72.
-
Unfinished Task Questionnaire was developed by the researchers from the literature review. It focused on the patient’s future goals and unfinished life tasks. It is comprised of 6 items with a four-level Likert rating scale, namely, not true (1 point) to exactly true (4 points). The total score ranged from 6 to 24; higher scores meant more unfinished tasks in the patient’s life. Cronbach’s alpha was .74.
-
General Perceived Self-Efficacy Scale (GSE) by Schwarzer (1997), translated by Sukmak et al. (2002). It focused on self-belief in her/his competence to succeed in difficult situation. It consisted of 10 items; each item was arranged in a four-level scale. The scale options were not at all true (1 point) to exactly true (4 points). Total scores ranged between 10-40 points. The high scores meant high levels of general perceived self-efficacy. Cronbach’s alpha was .74.
-
Family Relationship Questionnaire by Kaewsakulthong (2009) with 10 items. Each item had a five-level rating scale as follows: 1 = never to 5 = always. Total scores ranged from 10 to 50. A high score meant good family relationships. Cronbach’s alpha was .89.
Data collection
This study was reviewed and approved by the Research Ethics Review Committee for Research Involving Human Research Participants COA No. 319/2018, IRB No. 081/61, No. 230_2018T_OUT560 and No. 2561/201 project code ID 03-61-29Y. The researchers collected the data after receiving permission from the Committee. The data were collected during May 30-August 10, 2018 from Monday to Friday of each week. The researchers selected participants in accordance with the criteria reported above. There were 135 participants who read and answered all the questionnaires by themselves, which took around 15-20 minutes. One hundred and seven participants had difficultly reading by themselves. So, the researchers read all items for them and the participants documented the answers.
Data Analysis
SPSS Version 17.0 was used for analyzing the data of this research, and the statistical significance level of all tests was found to be < .05. The participants’ personal data was analyzed using descriptive statistics. Pearson’s product moment coefficient of correlation and Point-biserial correlation coefficient were used to analyze the relationship of the variables, and stepwise multiple regression analysis was used to analyze the predictors of death acceptance. All variables passed the test for assumptions of Pearson’s product correlation and linear multiple regression.
Results
Personal Information
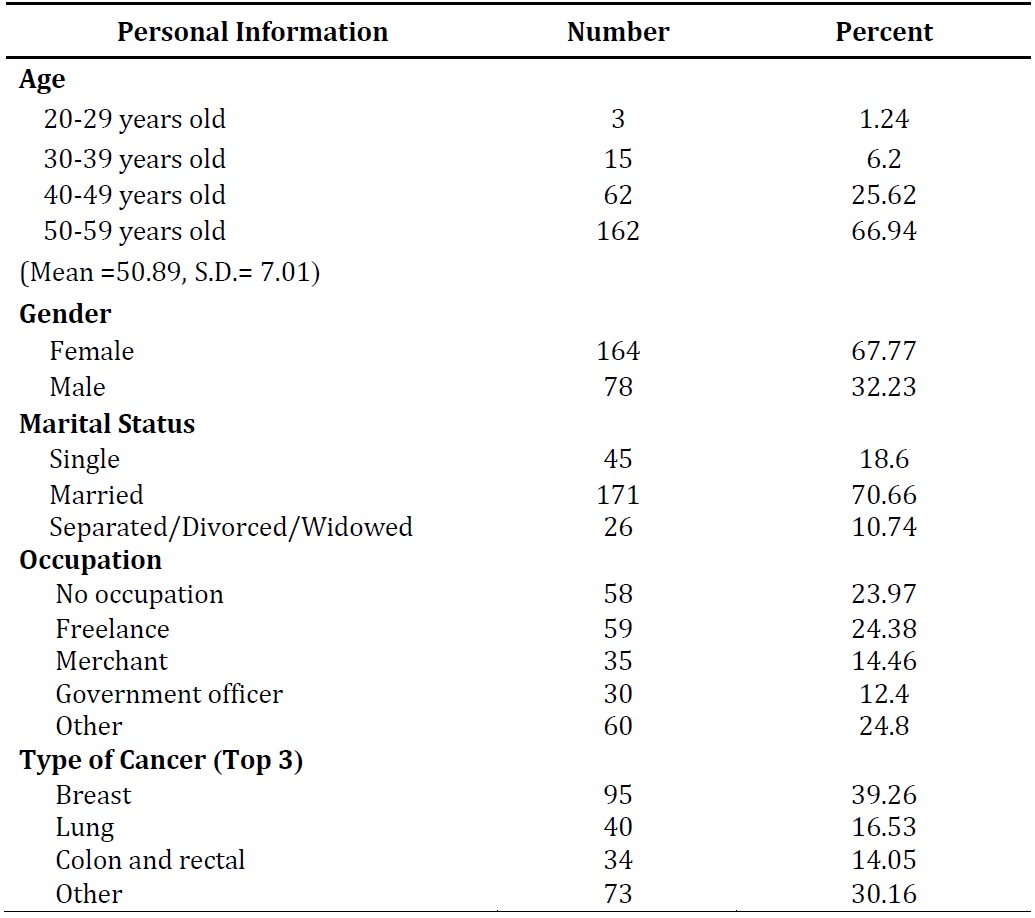
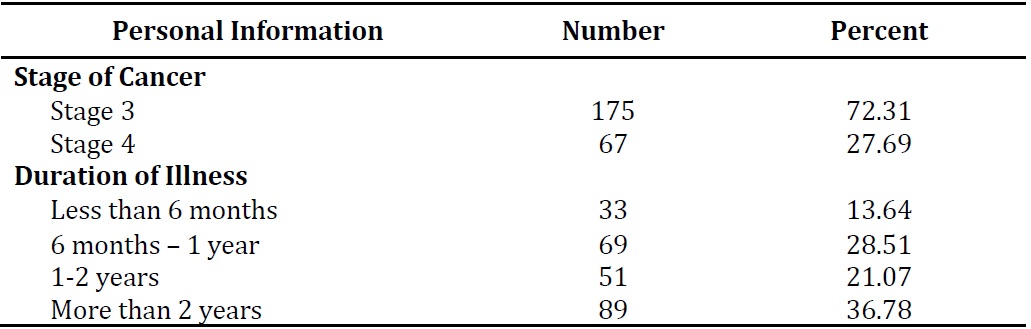
The participants consisted of 242 advanced cancer patients mostly aged between 50-59 years old (66.94%) with the mean age of 50.89 years (S.D. = 7.01). Most of the participants were female (67.77%) and were married (70.66%). The most common type of cancer was breast cancer (39.26%) and the majority of them were at stage 3 (72.31%). The duration of their cancer illness was more than two years (36.78%) (see Table 1).


Death Acceptance of Advanced Cancer Patients
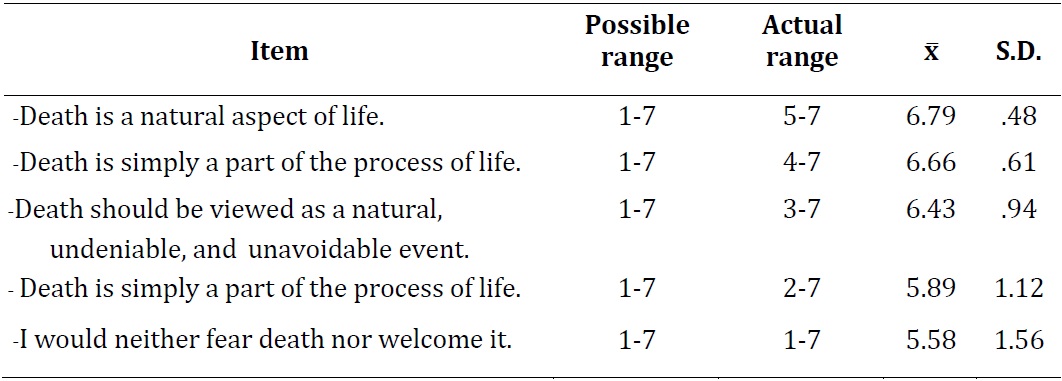
This present study found that the advanced cancer patients had high levels of death acceptance (mean = 31.22; S.D. = 3.59), and mean score of each items were as follows in Table 2.

Correlation Between Select Factors and Death Acceptance
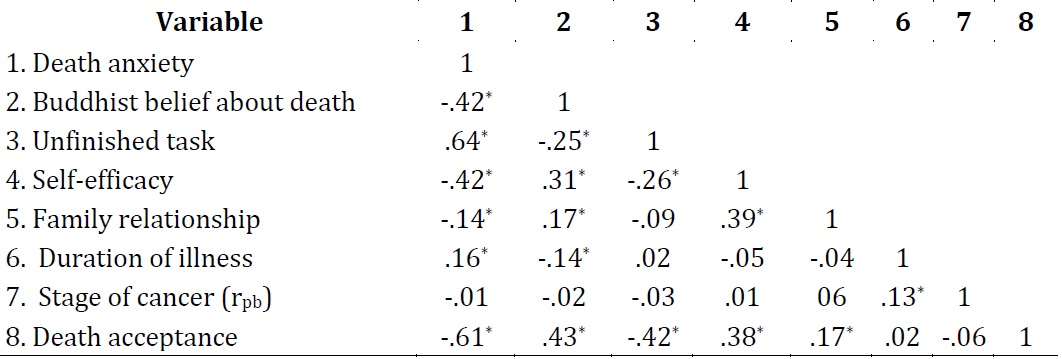
Pearson’s correlation and point biserial correlation showed that death anxiety and unfinished tasks were significantly negatively related to death acceptance (r = -.61, -.42, respectively; p < .05). However, Buddhist beliefs about death (r = .43, p < .05), self-efficacy (r = .38, p < .05), and family relationships (r = .17, p < .05) were significantly positively related to death acceptance. Duration of illness and stage of cancer had no relationship with death acceptance (see Table 3).

Stepwise multiple regression analysis was used to examine factors contributing to death acceptance. Table 4 shows a total of 42% variance of death acceptance to be explained by death anxiety, Buddhist belief about death, and self-efficacy. These results revealed that participants who had low death anxiety, more positive Buddhist beliefs about death, and higher self-efficacy could perceive and express their death in a better way.

Discussion
This study found that patients with advanced cancer had a high level of death acceptance that wasn’t congruent with Pinquart et al. (2006). This may be due to the fact that most of the participants were female, knew their diagnosis of advanced stage cancer, and all were Buddhists. Buddhists’ principle about “the three characteristics of existence,” which are suffering (dukkha), impermanence (anicca), and non-self (anatta) help people awareness about death and death preparedness (Rangsikosai et al., 2013; Visalo, 2009).
This present study found that a total of 42% variance of death acceptance was explained by death anxiety, Buddhist belief about death, and self-efficacy. Death anxiety was the strongest predictor of death acceptance among advanced cancer patients. The reason might be that advanced cancer patients in this study were most likely to have been treated for a period of 2 years or more. At present, patients are continuously treated and receive information about the disease continuously. So they can adapt to their diagnosis and learn about death, and as a result, death anxiety is low. When they had low levels of death anxiety, as a result, they can learn and understand the meaning of life and effect of their good attitude towards death, and so they can accept death (Rangsikosai et al., 2013). Patients with low levels of death anxiety can accept death (Sripa, 2011). The results of this study were consistent with Harding et al. (2005) who studied the relationship between death anxiety and death acceptance in Episcopal Christians in New York. Their study found that patients with a high level of death anxiety would have a low level of death acceptance. Stated another way, there was a negative relationship between death anxiety and death acceptance. Furthermore, findings from this study were consistent with Durlak and Kass (1982) who found that death anxiety had a negative relationship with death acceptance.
This study found that Buddhist beliefs about death had a positive relationship to death acceptance at a medium level and could predict death acceptance. This suggested that Buddhist beliefs can provide an understanding of death based on religious principles. Beliefs concerning death can help a person accept death (Corr et al., 2013; Tongprateep, 1991/2009). In this research, all of the participants were Buddhist and believed the cycle of birth and death is due to their own karma. In addition, they believed that all living things follow the laws of nature. Therefore, Buddhist beliefs about death can help people to understand the truth of life, let go, understand death, and mentally prepare to be acquainted with death and accept it (Rangsikosai et al., 2013; Visalo, 2009).
Though these findings reflected an Asian/Eastern perspective, research results were consistent with the study of Pinquart et al. (2006), which found that religious belief about death had a positive relationship with regards to death acceptance and could predict death acceptance. In addition, this study was congruent with the study of Harding et al. (2005), which found that theological religious factors had a positive relationship with death acceptance and that the belief in God and the belief in an afterlife had a positive relationship with death acceptance and could predict death acceptance.
The present study found that self-efficacy had a positive relationship with death acceptance and could predict death acceptance. According to Bandura’s Social Cognitive Theory, perceived self-efficacy is self-belief in one’s own competence to succeed in difficult situations (Bandura, 1997). The patients who had higher perceived self-efficacy would be able to assess and recognize that they could control and manage their difficulties including fear of pain, other symptoms, anxiety, fear, and facing death (Hirai et al., 2002). They could adapt to a threatening event and be ready to face near death and had better death acceptance. This study is consistent with Daaleman and Dobbs’s study, which found that self-efficacy, was significantly positively related to death acceptance (Daaleman & Dobbs, 2010).
Conclusion
This study found that a total of 42% of the variance of death acceptance was explained by death anxiety, Buddhist beliefs about death, and self-efficacy. Results indicated that better death acceptance was explained by low death anxiety, stronger Buddhist beliefs about death, and higher self-efficacy. Nurses should be aware of this crucial evidence for improving nursing programs to help patients with advanced cancer perceive a good death acceptance by decreasing negative factors (death anxiety) and increasing positive factors (Buddhist beliefs regarding death and self-efficacy).
Limitation of the Study and Recommendations
This study used the Death Acceptance Scale that was developed from Western culture and used only one dimension of the whole scale. Therefore, it might be necessary to develop the scale based on Eastern culture, especially Buddhist principles
Biographical Notes
Maliwan Krapo, R.N., B.S.N., is a master student in the Faculty of Nursing, Chulalongkorn University, Thailand. She worked as a research assistant on the “Palliative Care based on Buddhist Principle and Eastern Philosophy for Persons with Cancer” Research STAR. Her research interests include cancer patients and palliative care.
She can be reached at Faculty of Nursing, Chulalongkorn University, 254 Phayathai Road, Pathumwan, Bangkok 10330 Thailand or by e-mail at one_sk2@hotmail.com.
Sureeporn Thanasilp, Assoc. Prof., D.N.S., R.N., is Associate Professor in the Faculty of Nursing, Chulalongkorn University, Thailand. She worked as a researcher on the “Palliative Care based on Buddhist Principle and Eastern Philosophy for Persons with Cancer” Research STAR. Her research interests include cancer patients, palliative care, and chronic illness patients.
She can be reached at “Palliative Care based on Buddhist Principle and Eastern Philosophy for Persons with Cancer” Research STAR, Faculty of Nursing, Chulalongkorn University, 254 Phayathai Road, Pathumwan, Bangkok 10330 Thailand or by e-mail at s_thanasilp@hotmail.com.
Janya Chimluang, Assist. Prof., Ph.D., R.N., is Assistant Professor in the Faculty of Nursing, Chulalongkorn University, Thailand. She worked as researcher on the “Palliative Care based on Buddhist Principle and Eastern Philosophy for Persons with Cancer” Research STAR. Her research interests include cancer patients, palliative care, and chronic illness patients.
She can be reached at “Palliative Care based on Buddhist Principle and Eastern Philosophy for Persons with Cancer” Research STAR, Faculty of Nursing, Chulalongkorn University, 254 Phayathai Road, Pathumwan, Bangkok 10330, Thailand or by e-mail at chimnoko@yahoo.com.
Correspondence
The authors would like to thank Associate Professor Dr. Dawn Liam Doutrich for editing and proofreading this article. All correspondence concerning this article should be addressed to Sureeporn Thanasilp by email: s_thanasilp@hotmail.com.
Date of Submission: 2018-10-25
Date of the Review Result: 2018-11-12
Date of the Decision: 2018-11-15