

The number of people living long lives is increasing around the world, including in Thailand, which also has a growing elderly population. The number of older persons (defined as aged 60 and over) in Thailand has grown rapidly and will continue to do so in future decades. Since 1960 the number of older people has increased from approximately 1.5 million to 10.7 million in 2015 or 16% of the total population. Future population aging will occur even more rapidly with the number of older persons projected to increase to over 20 million by 2035 (Knodel et al., 2015). Age impacts both physical and psychological changes that influence mental health. Resilience is a positive function state that is correlated with a healthy state of mental health despite adverse life events. Resilience indicates one’s capacity to recover from extremes of trauma and stress (Davydov et al., 2010). The elderly who have high resilience are better able to deal with suffering and maintain a healthy state of mental health, whereas the elderly who have low resilience often have mental illnesses. Resilience was positively correlated to positive indicators of mental health (Hu et al., 2015) including being the strongest predictor of mental health (Wells, 2009).
One important factor that needs to be considered is the individual differences in the way people deal with challenges and stress. Therefore, measuring resilience means measuring an individual’s ability to successfully adapt in a crisis, including physical and emotional adjustment, social interaction, active coping, and alternative coping. Its outcomes are being able to withstand an adverse life event without manifesting mental health problems. However, few studies have reported on the elderly population and resilience (Felten & Hall, 2001; Rowe & Kahn, 2000; Wagnild, 2003; Wagnild & Young, 1993). The gaps in knowledge include resilience and a measurement tool that focuses on the elderly. Thus, there is a significant rationale underlying the development of a resilience scale for elderly Thai people. Measuring the strength of the elderly who are at risk is vital in assisting older adults dealing with major suffering. The process of successful adaptation among elderly people who are resilient can guide other elderly people to thrive in the same crises. So, the development and psychometric evaluation of the Thai Elderly Resilience Scale (TERS) is needed. The newly developed measure would help in assessing resilience, that is, the abilities and assets of the elderly Thai population despite adverse life events. Ultimately, the promotion of mental health and the prevention of mental health problems for elderly Thai people who are at risk can be improved.
Background
The conceptual framework for this study was constructed on a conceptualization of Thai elderly resilience and a norm reference framework. A definition of resilience is the ability to bounce back to normal life and remain mentally healthy in the face of adverse life events. The concept drawn from various studies includes: resilience involves a fluid process in which behaviors, thoughts, and actions can be learned and developed by anyone at any time (American Psychological Association, 2004); resilience encompasses physical and psychological function (Talsma, 1995), reflects relationships among individuals, family, and community (Tusaie & Dyer, 2004), and depends on personal strengths, lifestyle, and socio-cultural background (Ryff et al., 1998; Staudinger et al., 1993).
The framework was developed twice, initially as pre-specified domains and later as specified domains. The pre-specified domains were initially conceptualized through the three sources of resilience features based on (Grotberg, 1995, 2003): 1) “I HAVE” (external support) 2) “I AM” (inner strength) and 3) “I CAN” (social and problem-solving skills). These features were originally developed within a children-focused study, which was part of an international resilience project. The study was conducted in 30 countries including Thailand. In addition, it has been often been adopted by research in the Thai context (Kittivongvisut, 2001; Lhimsoonthon, 2000; Somchit, 1998; Takviriyanun, 2008). The pre-specified domains were synthesized with knowledge and empirical indicators from literature reviews (Connor & Davidson, 2003; Kinsel, 2004; Resnick, 2008; Takviriyanun, 2008; Wagnild, 2003).
Objectives of the Study
-
To develop an instrument to measure resilience in elderly Thai people
-
To conduct a psychometric evaluation of the new instrument
Methodology
The study was conducted through two main stages as follows:
1. The development stage is processed as domain identification, item generation, and scale format determination. Three sources of resilience labels by Grotberg (1995) “I Have,” “I Am,” and “I Can” were used as first identifier domains.
2. Psychometric properties testing based on DeVellis (1991) as follows:
Content Validity Evaluation
This study invited seven experts specializing in various areas relevant to the study: one geriatric nursing expert, one mental health expert, one psychiatric nursing expert, one geriatric psychiatrist, one psychologist, one researcher experienced in the development of a scale of resilience in adolescents, and one American professor working as a mental health nurse practitioner. The experts were asked to use a rating form, consisting of a four-point Likert-type scale, namely, 1=not relevant, 2=somewhat relevant, 3=quite relevant, 4=exactly relevant and to rate the relevancy of each of the 50 items. Moreover, they were asked to evaluate clarity and conciseness, using yes or no responses on each item, and were also invited to make comments on any items that seemed ambiguous, unclear, or inappropriate. The content validity was calculated based on the Content Validity Index (CVI). The CVI for the entire instrument is the proportion of the total items judged as content valid (Lynn, 1986). A CVI greater than or equal to 0.80 can be accepted (Waltz et al., 2005). In order to assess the content validity of each item and the overall TERS, items that were rated at level 3 or 4 on the relevance scale were retained while those rated with lower numbers were deleted. However, unacceptable items were discussed with the advisor(s) for modification. A re-evaluation based on the experts’ assessment was made to ensure the scale’s content validity. The second draft of TERS was thus achieved in this step.
Face Validity Evaluation
To determine the comprehensiveness of each item and the practicality of completing the scale, five elderly Thai people, who have various education levels, ages, gender, and marital status, were purposively selected as participants. They were asked to review the first draft of the TERS and respond to the comprehensibility, that is, their ability to understand, of each item and the practicality of completing the scale. Finally, a modification was made to create the second version while ensuring the comprehensibility and practicality of the TERS.
Pre-Testing
According to Polit & Hungler (1999), at least 30 subjects are appropriate for pre-testing. Thus, 30 Thai people aged 60 years or older who had recently experienced at least one adverse life event were selected for the study. The adverse life events of respondents included losing their home, living with cancer, loss of a loved one within the past month (e.g., husband and son), taking care of two family members suffering from mental illness, and living in poverty. The subjects were asked to rate the questionnaire by themselves. Those who were unable to respond to the questionnaire due to certain functional limitations, such as illiteracy, were read to by the investigator and then allowed to select the rating of choice on their own. Item analysis is one of the statistical procedures that allow an examination of the pattern of responses to each item that provides guidelines for revision. In this study, the alpha correlation of item to item, item to subscale, item to total scale, subscale to subscale, and subscale to total were analyzed. Whether to be retain, revise, or delete the items was considered at this step. Internal consistency is concerned with the homogeneity of the items within a scale. The relationships among items are logically connected to the relationships of items to the latent variables, and high inter-item correlations mean the items are all measuring the same concept (DeVellis, 1991). This study used a coefficient alpha or Cronbach’s alpha as a measure of the reliability of the internal consistency to demonstrate that its items were highly correlated. All subscales and total scale were calculated for Cronbach’s alpha coefficients.
Field-Testing
The sample for this step included the elderly people without psychiatric disorders residing in various settings, e.g., shelter homes, outpatients of primary care units (PCUs), chronic illness clinics, and outpatients of psychiatric hospitals, as well as residents of disaster-affected communities. Each represented a variety of mental statuses. The elderly who had significant physical and psychological limitations, such as blindness, deafness, loss of speech, dementia, and moderate to severe psychiatric conditions, were excluded. The sample size was estimated based on statistical assumptions for the factor analysis which requires, at least 10 subjects for each item (Munro, 2005), a minimum of five subjects per item is needed for a psychometric evaluation of a new measure (Nunally & Bernsteing, 1994), and a sample of 100-200 are adequate for factor analysis because factors are distinct (DeVellis, 1991). In total, 517 subjects were deemed sufficient for field-testing.
The internal consistency estimate using Cronbach’s alpha coefficients of the total TERS and dimensions were calculated. The alpha coefficients of 0.7 are accepted as the minimum for a newly developed instrument (Nunally & Bernsteing, 1994). Using the Nunally and Bernsteing criteria (1994), the items of the TERS scores were analyzed: First, the criterion level used as a guide for identifying and discriminating was 0.3. Item(s) below 0.3 were removed from the scale’s item set. Second, the criterion for the inter-item analysis was an average correlation between 0.3 and 0.7, which was desirable. Lastly, the criterion in the item analysis was that the internal consistency estimate (alpha), should not decrease if the item was deleted (Ferketich, 1990; Merle, 1998). Prior to deleting the items that failed to meet the criteria; the semantic meaning of each item was reviewed with the scale descriptions.
In this study, Exploratory Factor Analysis (EFA) was used to develop the internal structure of the TERS item set. A principal components and varimax methods were used to extract and rotate the components. An eigenvalue equal to or greater than 1.0 was used as the criterion to extract the number of components. The items whose factor loading ≥0.45 were considered to have practical significance (Hair et al., 1998). Finally, the scores from the respondents were extracted to specify factors of the TERS. The fourth draft of the TERS was the result of this step and it was then further evaluated for its reliability and validity in the final testing.
Final Testing
Final testing was performed to further develop the TERS. The scale derived from factor analysis was used as the instrument in this step. Additional reliability and validity tests were confirmed, and internal consistency was assessed. Two groups of elderly Thai people were selected for testing. The first group consisted of 30 participants living with their spouse and children in their home. The other group consisted of 30 Thai participants living in a shelter home. A sample size of 60 subjects (30 for each group) was needed to achieve the power at the 0.8 levels and the alpha at 0.05 levels. The internal consistency of items was evaluated three times: pre-test, field-test, and final test.
Furthermore, stability evaluation using a test-retest method was included in the reliability evaluation.. A Pearson product-moment correlation coefficient was used as the estimate of stability. The closer the coefficient is to 1.00, the more stable the measurement. The subjects in this test were 30 elderly Thai people living in a community. They were asked to respond to the instrument twice in two weeks. The objectives of the method were explained to the subjects. After the data collection was finished at the first meeting, an appointment for the second data collection was then made. The scores obtained from both administrations at two different times were calculated and interpreted to determine stability. Moreover, the final draft of the TERS was tested for its internal consistency once more. The field-testing step included sample, and data collection. The scale derived from factor analysis was used as the instrument. The data analysis was performed using Cronbach’s alpha coefficients, with an acceptable alpha of 0.7.
Ethical Consideration
The human research in this study was approved by the Ethical Committee, Faculty of Nursing, Prince of Songkla University.
Results and Discussion
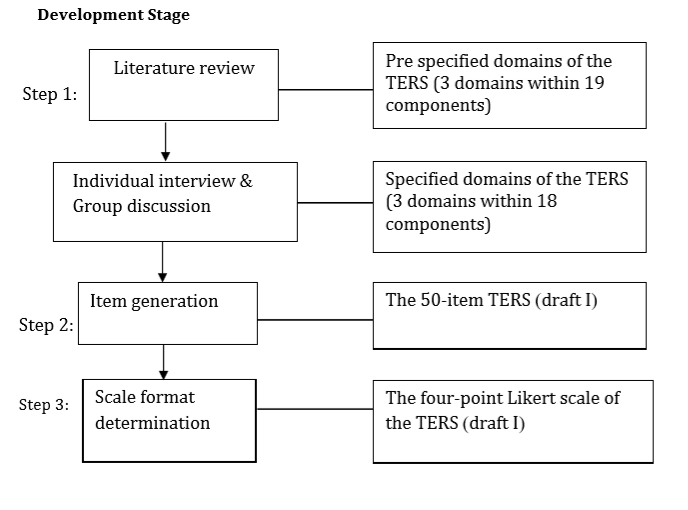
The findings from semi-structured interviews with fourteen elderly Thai people supported the initial three domains of the TERS. The TERS consists of 18 components in three domains: I AM, I HAVE, and I CAN. The first draft of the item pool, consisted of 50 items,. The first domain had 20 items with an indicator of I AM; the second domain with 15 items was an indicator of I HAVE; and third domain with 15 items was an indicator of I CAN (See Figure 1). This study used a 4-point scale where 1=not true, 2=somewhat true, 3=quite true, and 4=perfectly true.

Psychometric Evaluation Stage
A panel of six experts recommended content validity. After discussion, revision, and resubmission 2-3 times, a total of 47 items remained in the final scale. The CVI of the TERS draft II was .97, which indicated good content validity.
Face validity was evaluated by five elderly Thai people. The clarity and interpretability of the majority of scale items were confirmed, and minor rewording of scale items was recommended. The evaluators who could read took 15-20 minutes to complete the scale while another who could not read completed the questionnaire in 20-30 minutes.
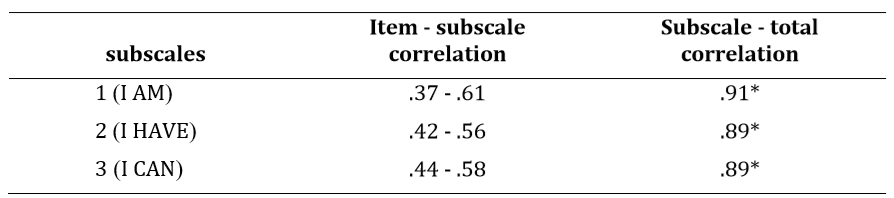
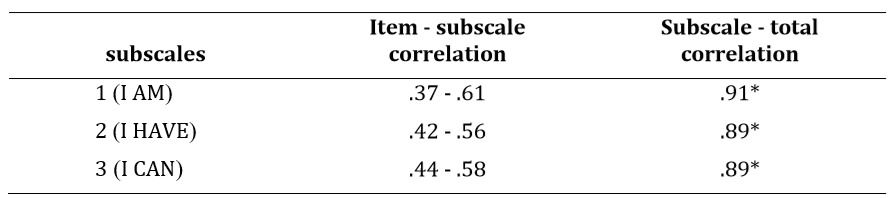
Field testing found that item to item correlation ranged from .002 to .53. As suggested by Ferketich (1990) and Nunally & Bernsteing (1994), item to item correlations should range between 0.3 and 0.7; therefore the items which had correlations lower than 0.3 were re-considered. The correlation of item to subscales among three scales ranged from .38-.61 for the I AM subscale, .35-.59 for the I HAVE subscale, and .26-.57 for the I CAN subscale. The correlation of items to total scale ranged from .21 to .58. The details of the four items which had a total correlations lower than 0.3, including the observation at the time of data collection showed that most respondents were confused and did not respond accurately. Those items were considered, and it was decided to delete them from the data set. The correlation of subscale to subscale was revealed as .705 (subscale of I AM and I HAVE), .710 (subscale of I HAVE and I CAN), and .706 (subscale of I AM & I CAN). The correlation of subscale to total scale ranged from .89-.91. The high correlation (r =.89 -.91, p < .01) indicated that each subscale measured a single concept (see Tables 1 and 2).
__42_items.png)
The item analysis revealed various sizes of correlation between items to items ranging from .002-.53, and many exceeded .30. However, there were five items that had the most correlations to others lower than 0.3. So, the items were dropped from the analysis at this point because they might not have measured the same underlying variables as the others. The remaining 42 item TERS were retained. Furthermore, the determinant of the 42-item correlation matrix was close to 0 (5.351-.070) which indicated that there might be several items that are strongly correlated to one another. These items were retained for factor analysis. Bartlett’s Test of Sphericity and the Kaiser-Meyer-Olkin measure of sampling adequacy (KMO) were then computed to confirm the appropriateness of applying factor analysis. The results of Bartlett’s Test of Sphericity was significant (χ2 = 7246.87, p=.00) and indicated high inter-item correlation. The KMO value of .932 was considered an excellent indication for using factor analysis. The commonality of all variables is necessary for it to be factorable; there were two variables that had a communality lower than 0.3. Therefore, the items were dropped from factor analysis. Finally, factor extraction was conducted on the 40-items.
A principal component analysis was selected as the factor analysis extraction technique. The goal of using this method was to convert a set of variables into a new set of variables that is an exact mathematical transformation of the original data (Munro, 2005). After extraction, the commonalities of the 40 variables ranged from .382-.663; eight factors with eigenvalues greater than 1 emerged from the analysis. For the overall factors, eigenvalues ranged from 1.051-11.415, total variances explained 53.44%. The first three factors consisted of 6-8 items, each of the fourth to seventh factors consisted of four items, and the ninth factor contained only two similar variables which were considered low-level in the hierarchy of factors. As noted by Comrey & Lee (1992), low-level factors seem to be less meaningful to the overall analysis. However, there is another criterion used in analyzing and interpreting the factor analysis, that is the scree test criterion (Cattell, 1966). Only five of eight met the scree test criterion. Factor rotation was run on the 40-item TERS.
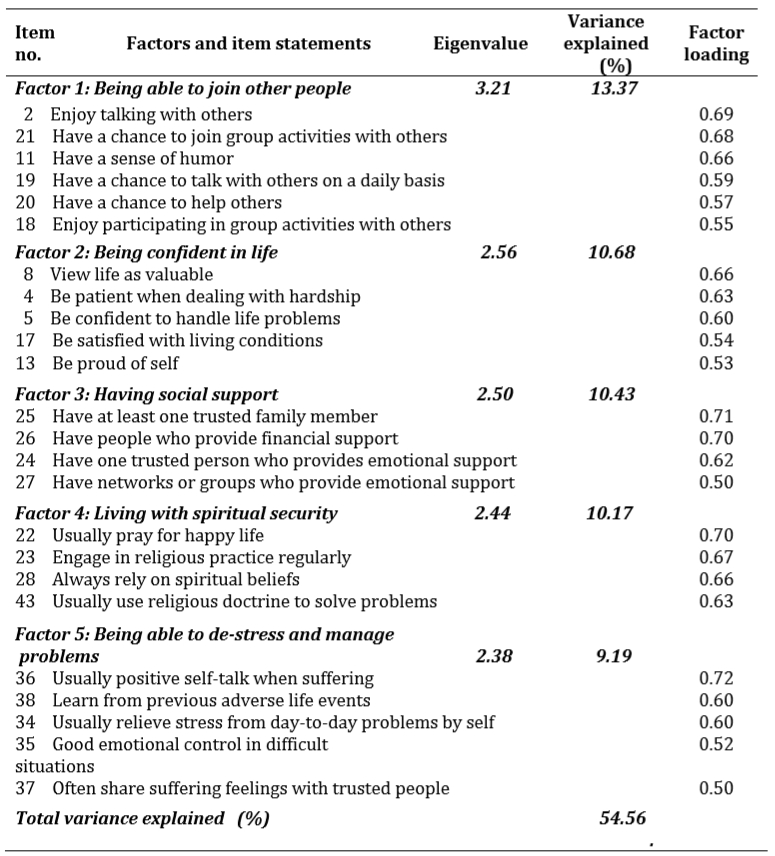
In addition, field-testing was performed using 517 elderly Thai subjects. The investigations found high internal consistency of the first draft TERS (α = 0.93), based on acceptable correlations between the item to item, item to subscale, subscale to subscale, subscale to the total, and item to total (r = 0.30-0.51). The results of Exploratory Factor Analysis (EFA) yielded the last version of the TERS consisting of 24 items categorized into 5 factors, i.e., 1) being able to join other people, 2) being confident in life, 3) having social support 4) living with spiritual security and 5) being able to de-stress and manage problems. The results of the Exploratory Factor Analysis are presented in Table 3.
.png)
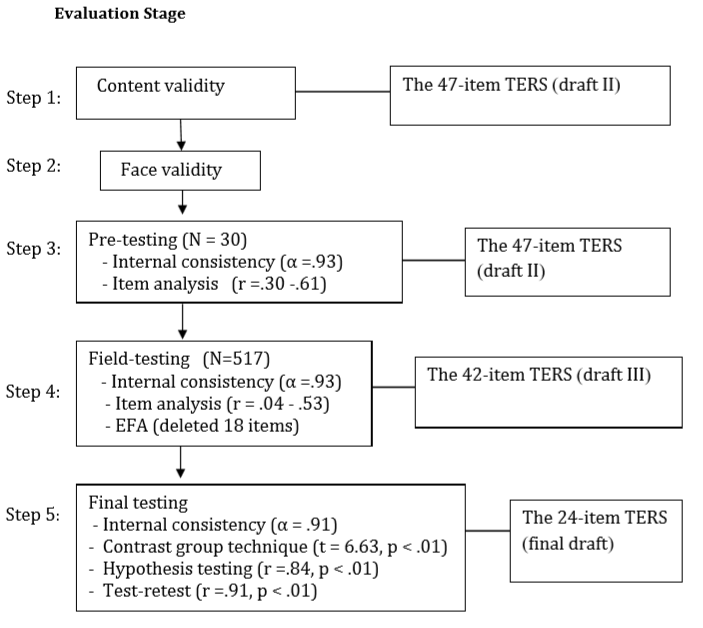
Final testing revealed a strong positive correlation between resilience and mental health scores (r=.84, p<.01, n=30). Known group comparison indicated the TERS was able to differentiate members of one group from the other by yielding a significant difference (t=0.33, p<.01) between mean TERS scores of the two groups of the elderly, one living in shelter homes (n=30), and the other living with their spouses and children (n=30). Both tests confirmed the construct validity of the scale. Furthermore, the stability evaluation using the test-retest method, by having 30 elderly Thai people complete the TERS questionnaire at two different times, demonstrated a high-level correlation (0.91) between the first and second administrations. The results confirmed the stability of the 24-item TERS. Moreover, the final testing of internal consistency yielded the alpha coefficient of total the TERS at 0.91, which additionally reflected high reliability. The overall results of the TERS developmental process can be seen in Figure 2.

.png)
Strengths and Limitations
The strength of this study lies in its theoretical foundation and its methodology. The underlying theories obtained from extant literature review and the qualitative data from the interviews of elderly Thai people were systematically processed and aligned. Furthermore, the methodology, including the step-by-step scale development, sample, instrument, data collection, and data analysis, emphasized the representation of Thai context, e.g., sampling included the elderly from all four regions of Thailand, considered Thai cultural values, etc. All of these effectively guarantee that TERS fits in the Thai context.
However, all studies have limitations, and this study is no exception. The generalizability of the research findings may be limited because the study sample was obtained through convenience sampling, including a greater representation of females (63.3%), which may affect the representativeness of the population. Another limitation of this study is that the number of stressors or the degree of adversity that people in this sample have faced was not specified; therefore, it was difficult to determine if all individuals viewed as resilient had experienced comparable levels of adversity in their lives. In addition, the review of the literature revealed that no prior theories, models, or ground information of elderly resilience in the Thai context were available to use as the theoretical framework for this study. Finally, this study employed a cross-sectional research design, whereas resilience is a dynamic developmental construct that can be developed over the lifespan and is affected by various factors. Therefore, longitudinal studies are recommended to follow the process of resilience in the case of individual resilience development.
Recommendations
Elderly resilience means the personal qualities that enable the elderly to rebound from adverse life events and go on with their lives. This study’s results show that Thai elderly resilience is fostered by positive interpersonal and intrapersonal characteristics, having social support and spiritual security, and the ability to cope and de-stress. Furthermore, the validity and reliability testing confirmed that the newly developed TERS can be used as a tool to assess the resilience level of elderly Thai people, especially for those at-risk of enduring difficult situations in life. Therefore, the conceptual structure of the Thai elderly resilience and the newly developed scale could have potential utility in both clinical practice and research,.
1. The understanding of the resilience in elderly Thai people could be an important benefit for the designing and implementation of nursing interventions to promote and enhance resilience in the aging population.
2. The new TERS could benefit nursing practice as it can be used to assess and detect early signs of mental health problems among the elderly.
3. The level of resilience gained from the assessment can provide valuable information on the risk of developing mental health problems among elderly Thai people. The appropriate intervention program can be built based on the needs and context of elderly people. Moreover, the scale will be useful in an evaluation of the nursing interventions by testing its effectiveness on the resilience level.
4. The resilience scale is not only useful for nursing practice but also beneficial for nursing research focusing on mental health among the elderly. Since this research disclosed the interrelatedness of the elderly resilience construct, future research aiming to develop nursing knowledge through testing a middle range theory of elderly resilience can be conducted. Nursing researchers will be able to use the emerging data in this study to explore the relative factors of resilience to gain an understanding of the reality of mental health among elderly Thai people.
Biographical Notes
Sonthaya Maneerat is a nursing instructor at Boromrajonani College of Nursing Nopparat Vajira,Bangkok Thailand. She has completed her PhD from the Faculty of Nursing at Prince of Songkla University, Songkla Province, Thailand.
She can be reached at Boromrajonnani College of Nursing, Nopparat Vajira, 681 Ramintra Street, Kannayao District, Bangkok, Thailand 10230, by phone at 66-8171-9540-4 or by e-mail at sonthaya@bcnnv.ac.th.
Sang-arun Isaramalai is an assistant professor. Currently, she works at the Faculty of Nursing, Prince of Songkla University, Thailand. She completed her Ph.D. in Nursing from University of Missouri-Columbia, United Stated of America. Sang-arun does research in cultural anthropology, medical anthropology, and medicine and public health nursing.
She can be reached at Faculty of Nursing, Prince of Songkla University, Songkla, Thailand 90110 or by phone at 66-8947-2938-0 or by e-mail at isangarun@hotmail.com.
Umaporn Boonyasopun is an assistant Professor. Currently, she works at the Faculty of Nursing, Prince of Songkla University, Thailand. She completed her Ph.D. in Nursing from the University of Maryland, Baltimore School of Nursing, United Stated of America.
She can be reached at Faculty of Nursing, Prince of Songkla University, Songkla, Thailand 90110 or by phone at or by e-mail at umaporn.b@psu.ac.th.
Correspondence
All correspondence concerning this article should be addressed to Sonthaya Maneerat at Boromrajonnani College of Nursing, Nopparat Vajira, 681 Ramintra Street, Kannayao District, Bangkok, Thailand 10230, by phone at 66-8171-9540-4 or by e-mail at sonthaya@bcnnv.ac.th.
Date of Submission: 2018-12-04
Date of the Review Results: 2019-01-22
Date of the Decision: 2019-02-23