Coronavirus Disease-19 (COVID-19) has altered everyday life around the world. On December 31, 2019, the Wuhan Municipal Health Commission of China reported that they found a cluster of cases of pneumonia in the city of Wuhan in Hubei Province that eventually turned out to be a novel coronavirus. The virus has spread to all corners of world, infecting more than 10 million people and causing more than 500,000 deaths (Treisman, 2020). The World Health Organization (WHO) officially declared COVID-19 a global pandemic on March 11 (Ghebreyesus, 2020). Rapid diffusion of the virus and a mounting number of deaths caused many countries to adopt drastic measures such as a total lockdown of an entire region or city, border closure, or blanket prohibition of entry against foreigners. In some countries, the society and the economy virtually ceased to function during the most severe phase of the crisis.
South Korea has employed a unique policy against the virus. It has never issued a city- or province-wide lockdown, quarantine, or curfew. South Korea resorted to an aggressive “track, isolate, and treat” approach. The Korea Centers for Disease Control & Prevention (KCDC) vigorously tracked down and tested every person who came in contact with someone who was infected. If a case was confirmed, the person who was infected received different treatment depending on the severity of the symptoms, ranging from treatment at home for those who showed very mild symptoms to intensive care in the hospital for the patients who needed it. Those whose test results were negative were ordered to stay at home in self-quarantine for 14 days. To identify persons who had been in contact with a person who was infected, the KCDC used personal information such as credit card transaction data, mobile location data gathered from the individual’s smartphone, and CCTV footage to track confirmed patients’ paths. The KCDC would then test everyone who has been in contact with the person who was infected. The KCDC also made information about the places visited by people who were infected publicly available. So far, it seems that the South Korean approach has worked, at least in containing the spread to a manageable level. The number of new confirmed COVID-19 cases remained at 46 cases a day during the last week of June, dropping dramatically from a peak of 909 new cases recorded on February 29.
Besides the government’s “track, isolate, and treat” approach and aggressive use of personal information, one notable aspect of the South Korean experience is a high level of compliance of the people with the government recommendations. Ever since the major outbreak in February, it has been, and still is, rare to find anyone without a mask on the street in South Korea. There has not been much complaint against possible privacy invasion nor have there been many reports about violations of self-isolation guidelines. Most South Koreans willingly followed the KCDC’s recommendations to wear masks when not at home, wash hands more frequently, disinfect widely, cut down on activities outside their home, etc. The question is what motivated South Koreans to readily follow the KCDC’s recommendations. This paper seeks to find the determinants of preventive behaviors by South Koreans during the COVID-19 outbreak. We used data collected from a survey on South Korean respondents, focusing on the relationship among individual’s anxiety over social safety, media exposure, negative emotions, and preventive behaviors. The main goal of the paper, however, is not to provide a rigorous theoretical explanation. Instead, the authors seek to draw practical and theoretical implications from the empirical data.
Literature Review
Faced with a pandemic outbreak, public health authorities seek to educate the public about the nature of the threat and necessary measures for protection. The public’s compliance with the government’s policy, however, cannot be guaranteed. For example, a study on a Dutch outbreak of H7N7 avian influenza reported that the public’s adherence to behavioral measures, such as wearing masks and goggles, was low (Bosman et al., 2004 as cited in de Zwart et al., 2007). Thus, understanding what motivates people to adopt preventive health actions is critical in combating a pandemic.
Risk Perception and Preventive Behaviors
Literature on the SARS coronavirus pandemic and on a potential human pandemic from the avian influenza virus (especially the H5N1 subtype) provides information about a population’s response to the threat of pandemics. One of the key determinants of the public’s response to the epidemic is perceived severity of the threat and personal vulnerability. Previous studies (Cava et al., 2005; Leung et al., 2003; Smith, 2005) found that a population’s willingness to comply with preventive behavior is closely related to the perceived threat of the SARS coronavirus. Lau et al. (2003) reported that use of hygiene measures increased rapidly during the first phase of the epidemic when the perceived threat was great. Di Giuseppe et al. (2007) found that, among the Italian population, those who perceived a higher risk were more likely to comply with hygiene recommendations. Research involving South Korean university students indicates that during an epidemic, such as MERS, Korean women perceived greater risk than men and that risk perception is related to preventive behaviors (Yang & Cho, 2017).
The perceived level of threat, however, does not ensure adoption of preventive behavior. Takeuchi (2006) reported that Thai farmers did not follow government recommendations against direct interaction with poultry even though they were very aware of the potential risks of H5N1 virus infection. The protection motivation theory argues that higher risk perceptions must accompany perceived availability of effective preventive measures and perceived self-efficacy (Rogers, 1975). In the case of the Thai farmers, they felt that they could not avoid direct interaction despite the government’s warning (Takeuchi, 2006). Perceived efficacy of preventive health actions affects people’s readiness to adopt prevent behaviors. Lau et al. (2003) found that those who perceived high efficacy of preventive behaviors, such as wearing a mask, frequent hand washing, and avoidance of public locations, adopted relevant protective measures more readily.
Emotions
Emotions have been shown to play a role in risk perception (Sjöberg, 2007). Emotions that lead to increased risk perception can also lead to increased behavioral compliance with recommendations, provided trust is present (Khosravi, 2020). A new measurement, the Fear of COVID-19 Scale (FCV-19S) has recently been developed (Ahorsu et al., 2020). Pakpour & Griffiths (2020) have explained the importance of understanding the perception of fear as a motivator for preventive behaviors. Some evidence from various countries already shows the connections between risk perception and behavior (Dryhurst et al., 2020). One study using the FCV-19S found that fear was the only factor related to preventive behaviors (Harper et al., 2020). This scale has already been used to consider fear of COVID-19 in other countries, such as India (Doshi et al., 2020) and Cuba (Broche-Pérez et al., 2020). While this 7-item scale was not yet known to us when the questionnaire for our study was made, some of the emotions or signs of emotions in this scale, including insomnia and fear, are similar to items used in our study.
Mass Media Risk Communication
In a crisis such as a natural disaster, effective communication plays an important role (M. Lee, 2008). The public use media more frequently to gain updated information. Background information supplied by the media helps the people to better understand the causes, impact, and aftermath of a natural disaster (Ali, 2013). Communication researchers have regarded the mass media as a key dissemination channel for risk messages and emergency information during a catastrophe. People faced with external hazards require timely and accurate information from the authorities in order to make informed decisions and protect their personal well-being (Lowrey et al., 2007). The mass media can create public awareness about risk as well as public policy priorities in regard to disaster management (Barnes et al., 2008).
During the initial phase of the SARS epidemic, the majority of Hong Kong residents followed the development of the disaster via traditional mass media, while the Internet played a relatively insignificant role in providing emergency-related information (Lau et al., 2003). Lau et al. (2003) argue that traditional types of mass media still play an important part in a public health crisis.
The role of the mass media during the current COVID-19 crisis appears to be as great as in any epidemic, if not greater, at least in South Korea. The KCDC has been holding daily press conferences to report the daily progress of the disease, to inform the people of public policy decisions, and to educate the public about better ways to protect themselves and others against the virus. The press provided daily updates largely based on the KCDC’s information, recommendations from medical experts, and the ongoing global progress of COVID-19. Whether media exposure of COVID-19 related information affected the public’s willingness to adopt preventive behavior, however, remains an empirical question.
Connection Between Media, Emotions, and Behavior
The connection between media exposure and behavior during the COVID-19 pandemic has been suggested by others (e.g., Mohammadi et al., 2020). Garfin et al. (2020) warned that, similar to what happened during the Ebola and H1N1 outbreaks, exposure to media, especially graphic media, could increase stress and anxiety. Similar connections have been found in other pandemics as well. For example, in surveys from the Netherlands, high anxiety and attention to media information about the Influenza A (H1N1) pandemic were both associated with taking preventive measures (Bults et al., 2011). A study from Japan related to risk perception of nuclear radiation after the Fukushima incident found a positive relationship between trust in the media and risk perception and from risk perception to anxiety (Guo et al., 2017). Wu & Li (2017) found that “personal risk perception mediates the effect of mass media exposure on precautionary behavior” regarding the haze issue in China.
Gender and Age
Gender, age, and other demographic variables can have an effect on risk perception and behaviors in a pandemic. During the H1N1 epidemic of 2009, although both male and female university students in South Korea increased the frequency of hand washing, females were found to wash their hands more than their male counterparts (Park et al., 2010). Lau et al. (2003) found that women and older people in Hong Kong were more likely to take precautions against SARS. This trend of greater risk perception among women has already been noted during the COVID-19 pandemic, including in a 10-country, 3-continent survey (Dryhurst et al., 2020). A recent survey from the USA found that women were more likely to intend to wear a face covering, partly because they perceived a greater risk (Capraro & Barcelo, 2020). Cuban women experienced higher levels of fear of COVID-19 than men in one survey (Broche-Pérez et al., 2020). Another study from Saudi Arabia found that women and older people were more likely to follow the recommendations for preventing the spread of COVID-19 (Al-Hanawi et al., 2020). However, age has not been a consistent factor across all countries; in Ethiopia, those in their 30s were the most likely to take preventive measures, while those in their 40s were the least likely to (Kebede et al., 2020).
Various explanations have been suggested for these effects. Some may be physiological. For example, Liu et al. (2020) discussed differences in the reactivity in neural networks between men and women when facing fear. Other explanations may be more practical: many childcare centers and schools closed at least temporarily due to COVID-19, and mothers are more likely than fathers to be responsible for childcare under these circumstances (Alon et al., 2020).
Health
One additional variable we looked at was health. People with certain health conditions are more likely to experience severe complications related to COVID-19 (CDC, 2020a). In one large survey from China, people with diabetes were more likely to rate their health as poor and to perceive a higher risk related to COVID-19 (Yan et al., 2020). Also worth noting is a relationship between health and positive emotions (e.g., Kok et al., 2013). Therefore, the relationship between self-reported health, risk perception, and behavior seems worthy of consideration.
Research Question
This study seeks to discover the determinants of preventive behavior among the South Korean population during the COVID-19 pandemic. The focus of the analysis is on two types of variables: those related to anxiety over social safety against COVID-19, and those related to media exposure. In addition to the perceived threat of COVID-19, the authors investigate the roles of other variables such as negative emotions that a person may feel because of the situation, predictions regarding the future COVID-19 diffusion, health, sex, and age.
The research question of the paper is:
RQ: What are the determinants of people’s willingness to adopt preventive behaviors to slow the spread of COVID-19?
Methodology
Survey Data
The survey data used in this paper came from the Korean Academic Multimode Open Survey (KAMOS), a nationally representative, probability-based panel. KAMOS is similar to other probability-based online panels for which members are recruited via offline surveys (Blom et al., 2016). Cluster sampling based on geographical areas established by Statistics Korea (KOSTAT) was used to select the home addresses of potential panel members. The representativeness of KAMOS was tested by comparing the demographic variables of its initial sample in 2016 with the results of two other major surveys in South Korea. The representativeness of a subsequent online/phone survey of panel members was then tested by comparing the respondents’ demographic variables and the results of several repeated questions to the initial 2016 survey results (Cho et al., 2017). Additional panel members were recruited in annual face-to-face surveys conducted 2017-2019. The face-to-face surveys had a response rate of 50%-63% and were also representative in terms of gender, age, residential area, income, and education level. The panel now consists of 8,500 members who were invited to participate in a survey conducted March 24-April 25, 2020 either by the e-mail address they provided in the initial survey or by phone if they had indicated that they preferred to be contacted that way. A total of 1,011 panel members (11.9%) responded. Post-stratification weights, which were estimated on the basis of the population distributions of age, gender, and residential area, were applied to the data. A comparison of other demographic variables of respondents post-weighting (e.g., education, job, income, religion) between the 2020 respondents and the 2019 face-to-face panel recruitment respondents are similar. This suggests that KAMOS continues to be a nationally representative panel. The complete English translation and dataset is available online (KAMOS, 2020).
Measurements
We used questions regarding the increased frequency of hygiene behaviors, such as wearing masks, washing hands, cleaning/disinfection, and some social distancing behaviors, such as decreasing activities outside their home and canceling meetings, as measurements of preventive behaviors against COVID-19. All the questions, except those about wearing masks, used 5-point scales asking about the frequency of certain behaviors indicating whether they currently engage in behaviors more, the same, or less than usual. To measure compliance with the recommendation to wear a mask, respondents were asked about how often they wear a mask in crowded places (never, occasionally, often, always, it’s hard to say). Scores of wearing masks were weighted to have a maximum score of 5. We used the average of the five questions as the preventive behavior index score.
The answer to the question of “Do you or do you not usually feel anxiety about your social safety, such as security, disaster, environment, disease, and crime?” was used as the measure of respondent’s “anxiety about social security.” Perceived risk of COVID-19 infection was measured by a question that asked, “Do you think you are likely to become infected with COVID-19 or not?”
Media exposure was calculated by adding up time of exposure to TV and newspapers. Increased media exposure was measured by a self-reported assessment of increased time of exposure to TV and newspapers.
Emotions were calculated using a 5-point scale that asked respondents how often they experienced 11 different emotions due to COVID-19. Initially, we expected that fear would be the main emotion driving attitudes and behavior regarding COVID-19 preventive measures. However, after performing factor analysis, we discovered that eight of the emotions formed one dimension. Among the 11 emotions, these eight emotions were the ones that we would consider to be negative emotions: anger, annoyance, fear, sadness, anxiety, insomnia, helplessness, and stress. The unrelated three emotions were the positive emotions of excitement, calm, and confidence, which were not found to have to have a relationship with the dependent variables (see Table 2). Having found this relationship between the negative emotions, we decided to consider them as an index of negative emotions, using the average score of the eight negative emotions as the negative emotion score.
Health was measured on a 4-point scale, with 1 being “Not very good” and 4 being “Very good.” For the sex variable, male was recorded as 1, while female was zero.
Most of the variables showed normal distribution, making them adequate for a regression analysis. The only exception was mask-wearing behavior, which shows a high level of skewness (-4.975). Because there is no plausible way to normalize an item that was measured on a 4-point scale, no corrective action was taken to address the problem of skewness in mask wearing behavior. The combined score of preventive behaviors, the preventive behavior index score, did not have the same problem.
We used IBM SPSS Statistics version 26.0 for statistical analysis.
Results
Summary of Results
Preventive Behaviors
Among 1,008 valid responses (three respondents did not answer some of the questions), an overwhelming 94.3% reported that they wear masks in highly populated locations. A combined 91.4% of respondents wash their hands more frequently (slightly more 33.3%, much more 58.1%), and 61.4% of the respondents answered that they clean and disinfect more frequently since the beginning of the COVID-19 outbreak. Most of the respondents followed social distancing guidelines quite well; 82% of the respondents reported going out less frequently, and 90.7% of them also canceled all meetings (47.2%) or some meetings (43.5%).
Attitudes About Government
Overall, the respondents judged the government’s policy against COVID-19 favorably; 52% of the respondents answered that they were satisfied with the government’s reaction, while only 27.2% answered negatively. South Koreans evaluated the medical response of the government more favorably than the economic response; 69.9% of the respondents were satisfied with the medical policy, whereas only 30.9% of them showed a similar attitude towards the economic policy.
Media Exposure and Attitudes
Among the respondents, a total of 46.3% (much more, 11.4%; slightly more, 42.3%) reported increased exposure to traditional media. A combined 48.8% of the respondents reported their trust in the media has increased. This may due to people’s impression that the media provided the right amount of the information – 60.5% of the respondents answered that the amount of information provided by the media was adequate, while only 15.8% of them felt it was insufficient, and 23.7% reported that the amount of information was excessive.
Analysis of the Data
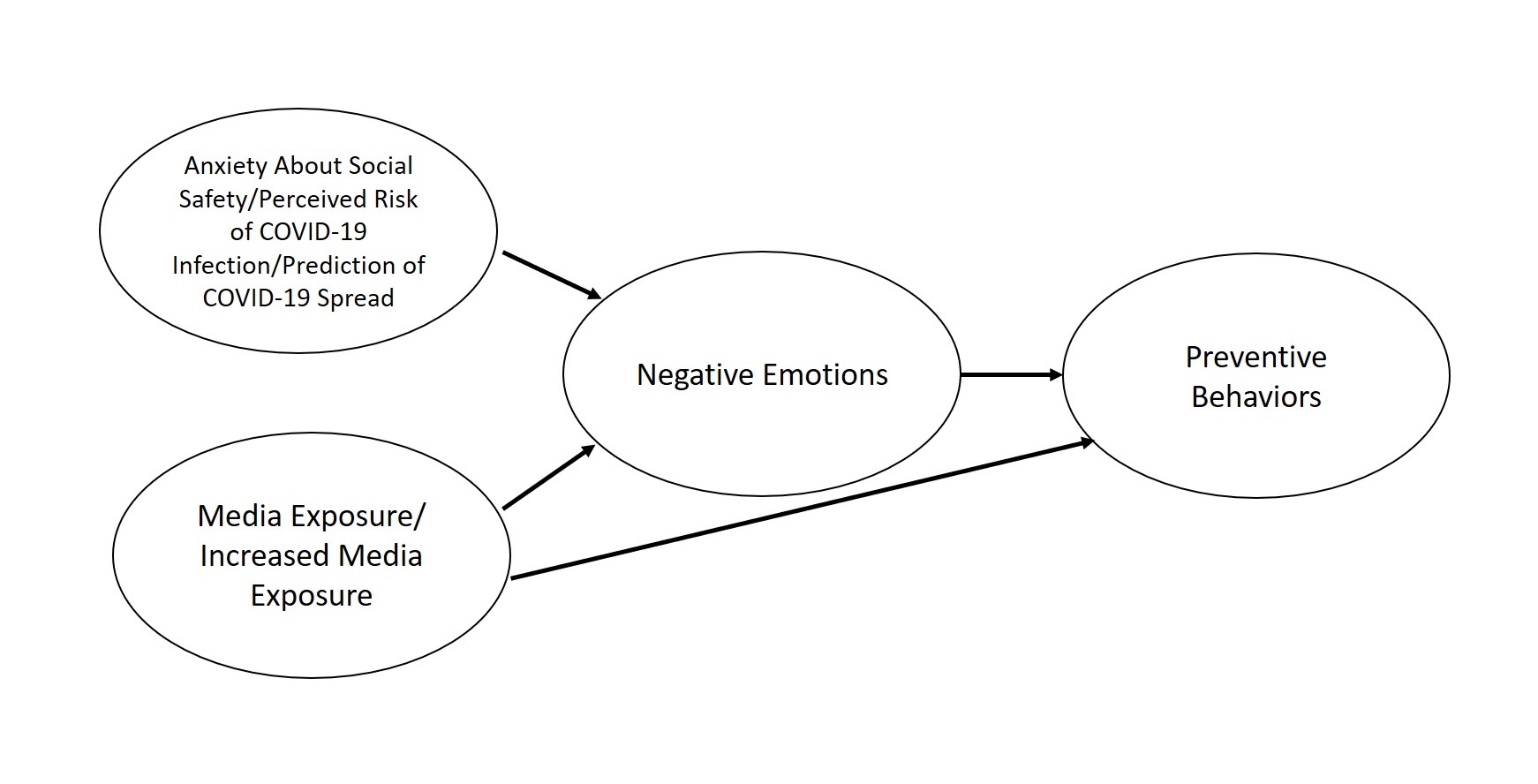
We theorized a multiple-step causal relationship between media exposure, negative emotions, and preventive behaviors against the COVID-19 virus. We conducted a series of regression analyses. First, we conducted a regression analysis to discover determinants on respondent’s negative emotions. In the next step, a set of regression analyses were carried out to assess the effect of negative emotions on preventive behaviors such as wearing masks, washing hands, and reducing the number of social gatherings. Additional regression analyses that employed each type of preventive behavior as dependent variables were conducted to acquire further information.
The first regression model included negative emotions as the dependent variable, and anxiety over social safety, perceived risk of COVID-19 infection, media exposure, increased media exposure, health, and prediction of COVID-19 spread as independent variables. The model also contained control variables that are related to socio-economic status; sex, age, education, and income. The model had an F value of 27.034, adjusted R2 of .212, and p-value of .001. All the independent variables and sex were found to have statistically significant relationships with the dependent variable. The directions of the relationship were not identical. Women were more likely than men to experience negative emotions (βo=-.134, p<.001) and those whose health was not very good were more likely to experience negative emotions compared to those whose health was better (βn=-.097, p=.001). Among the independent variables, anxiety about social safety had the strongest impact (βf=.286, p<.001) on negative emotions. Perceived risk of COVID-19 infection (β=.70, p=.023), prediction of COVID-19 spread (β=.121, p<.001), media exposure (βt=.063, p=.039), and increased media exposure (βn=.093, p=.001) were significant as well. Age (β=.054, p=.115), education (β=-.004, p=.894), and income (β=-.015, p=.611) did not have any significant relationship with the dependent variable.
The second regression model included negative emotions as an independent variable along with the other variables used in the previous regression analysis. The dependent variable was the preventive behavior index. The model had an F value of 12.990, adjusted R2 of .122, and a p-value of .001. As we predicted, negative emotions had a strong statistically significant relationship with preventive behaviors (βw=.220, p<.001). Variables such as health (β=.104, p=.001), media exposure (β=.097, p=.003), and increased media exposure (βn=.080, p=.01) had a significant effect on preventive behavior. In addition, the control variables of age (βc=.131, p<.001) and gender (β=-.103, p=.001), had significant relationships with the dependent variable as well. The other independent variables and control variables failed to show any statistically significant relationships with preventive behavior.
We conducted several additional regression analyses that had each type of preventive behavior as a dependent variable. Each analysis yielded quite different results. Media exposure was significant only on cleaning/disinfecting (β=.128, p<.001). Increased media exposure had a positive impact on washing hands (βo=.077, p=.018), cleaning/disinfecting (β=.077, p=.017), and meeting cancelation (β=.067, p=.039). Anxiety about social safety had no statistically significant relationships with any type of preventive behaviors. Perceived risk of COVID-19 infection had an effect only on meeting cancelation (β=.095, p=.005). Prediction of COVID-19 spread was negatively related to increased frequency of washing hands (β=-.078, p=.020). Interestingly, health was positively related to washing hands (β=-.092, p=.005) and cleaning/disinfecting (βa=.103, p=.002). Negative emotions had effects on each type of preventive behavior, except washing hands (β=.064, p=.073). A summary of the results is shown in Table 4.
Discussion of Findings
Overall, South Koreans appeared to have followed the government’s recommendations on preventive measures relatively well. As noted above, over 90% of respondents wear masks, wash their hands more frequently, and have canceled at least some meetings. Given that those preventive measures were presented to the public as recommendations rather than as mandatory government orders with accompanying penalties, the level of compliance by South Koreans is notable.
The increased use of traditional media at this time may be explained as follows: Faced with a highly uncertain and risky situation, South Koreans seem to have responded with more active information seeking to evaluate the situation and the degree of risk to their own safety and to acquire useful tips on preventive actions. The increased media exposure may also account for the increase in trust in media. People’s impression that the right amount of information was provided may also affect their trust in the media. The correlation between the people’s impression on the amount of information and increased trust in the media was significant, although it was weak (r=.06, p<.05).
The purpose of this paper is to determine what motivated South Koreans to adopt preventive behaviors towards COVID-19 virus. From the survey data, we were able to find some patterns of the effects. The strongest predictor of preventive behaviors was negative emotions, which had the largest βh (.22) among the independent variables. Negative emotions themselves were influenced most strongly by the respondent’s anxiety over social safety (βo=.286), followed by prediction of COVID-19 spread (βC=.121). In other words, respondents felt stronger negative emotions if they are usually anxious over social safety and predicted a worse scenario regarding COVID-19 diffusion. On the other hand, males (β=-.134) and those who felt healthier (β5=-.097) experienced fewer negative emotions. Media exposure and increased media exposure both have significant relationships with negative feelings. We can conclude that people increased media usage during the COVID-19 crisis, and exposure to large amounts of COVID-19 news led them to experience more anger, annoyance, fear, sadness, anxiety, insomnia, helplessness, and stress.
According to the data, media exposure, increased media exposure, health, and sex seem to have both a direct and indirect effect on adoption of preventive measures. All four variables mentioned above had significant relationships with both negative emotions and preventive behaviors. Meanwhile, individuals’ attitude variables—such as anxiety over social safety, perceived risk of COVID-19 infection, and prediction of COVID-19 spread—have significant relationships with negative emotions, but not with preventive behaviors. The results show that these attitudes affect preventive behaviors only indirectly through negative emotions.
Health had a negative relationship with negative feelings. However, it had a positive relationship with preventive behavior. The findings suggest that those who felt healthier experience fewer negative emotions, but were more willing to adopt preventive behaviors. A number of studies have found that positive emotions are associated with physical health and longevity (e.g., Kok et al., 2013). The positive relationship with preventive behavior may be because healthy people are healthy because they are more likely to accept these kinds of hygiene recommendations. On the other hand, it might be because if someone is very unhealthy, some of the recommended behaviors may be harder to adopt. For example, a person with a breathing disorder may have a difficult time wearing a mask for a long period of time or a person with frail skin may have problems with excessive hand washing. More research is needed to provide a more persuasive and conclusive explanation about this finding.
From the results of regression analyses we can identify two major types of determinants of preventive behaviors. The first type of determinants are variables related to individuals’ fear of personal safety regarding COVID-19—anxiety over social safety, perceived risk of COVID-19 infection, and prediction of COVID-19 spread—which affect prevention behaviors only through negative emotions. Another type of determinants are variables related to media exposure, which have both a direct and indirect impact on the adoption of preventive measures. This conclusion agrees with the traditional theoretical understanding in media effect research in that there are two main types of determinants of personal behavior: personal traits and media exposure.

The direction of the relationship between negative feelings and media exposure may be bidirectional. That is, more exposure to negative news on COVID-19 may lead a person to feel stronger fear, anxiety, anger, sadness, helplessness, and so on. In turn, those who came to feel more negative emotions may seek more information to find a way to better cope with the situation and their emotions. A future study is necessary to find a more conclusive answer.
In addition, preventive behaviors related to social distancing may also cause stronger negative emotions. The American CDC warns that social distancing may make people feel isolated and lonely and results in increased stress and anxiety (CDC, 2020b). The WHO also notes similar negative emotional consequences of isolation (WHO, 2020). Due to the limitations of the data, the current study is unable to provide more insight. A future study will have to address the issue.
Similar to the findings in previous research (e.g., Lau et al., 2003), we found that females are more likely to engage in preventive behaviors. However, our data suggests that female respondents tend to clean and disinfect more frequently and are less likely to go out, while previous research found that females were more likely to wear mask, to wash hands, and tend to stay at home. The same research found a significant association between age and preventive activities such as washing hands, disinfection, and avoiding crowded places. In our South Korean sample, age was significantly related to behaviors of washing hands, going outside less frequently, and canceling meetings, which makes sense given that age was widely reported to be related to the severity of COVID-19.
Conclusion
We tried to ascertain the determinants of preventive behavior adoption among the adult South Korean population, relying on survey data. From the analysis, this study was able to show that the effects of personal attitudes towards the COVID-19 crisis affect negative emotions, in particular, anger, annoyance, fear, sadness, anxiety, insomnia, helplessness, and stress, which in turn triggers adoption of preventive measures. We have confirmed that the connection between perceived risk of COVID-19 and compliance with preventive behaviors that was identified by others working in various countries (e.g., Ahorsu et al., 2020; Harper et al., 2020) also exists in South Korea. In addition, we have expanded the range of negative emotions that may be connected with each other and with this kind of effect. While the previous research on fear already includes some of the other negative emotions that we found to be connected, such as insomnia (Ahorsu et al., 2020) or anxiety about COVID-19 (e.g., S. A. Lee, 2020), our identification of eight negative emotions that were connected and impacted behavior may expand the understanding of the manifestations of fear or anxiety in general or about pandemics in particular. Future research could confirm whether this set of negative emotions behave as a single factor in a similar way in other countries or under other conditions. Increased awareness that feelings like annoyance, helplessness, or anger are also connected with fear and behavior, either as additional symptoms and manifestations of fear and anxiety or as part of a broader collection of negative emotions, may be useful to mental health professionals, health communicators, and others trying to understand emotions and their role in human behavior in times of crises, like a pandemic, or in general. Our finding that risk perception was not directly related to preventive behaviors, but instead affected emotions, which in turn affected preventive behaviors, was different from the impact of risk perception seen elsewhere. It increases our understanding of the relationship between risk perception and behavior, and this relationship, mediated through negative emotions, should be tested in other countries and in other risk perception situations.
In addition, this paper was also able to demonstrate the significant role of the media on negative emotions as well as on preventive behaviors. According to the findings, exposure to COVID-19 related information may cause a person to feel stronger negative emotions, which increases their likelihood of preventive behavior adoption. While it can be argued that media coverage of a pandemic may not be beneficial to mental health issues that are byproducts of the pandemic, as suggested by Garfin et al. (2020), information on the pandemic disseminated by the media can play a positive role in protecting people’s physical health by causing them to adopt preventive behaviors. This is consistent with other findings about the role the media plays in a pandemic or in other crises (Lau et al., 2003).
We focused only on traditional media such as TV and newspapers. This paper has not addressed the role of social media, which have become important sources of news and which are also a major conduit of social support. The role social media played during the COVID-19 pandemic can be an interesting topic to explore in a future study.
Even though we discovered some of the main motivators of preventive behavior adoption among South Koreans, it is still unclear why South Koreans have been more willing to follow government recommendations compared to populations in other countries. A comparative study is required to answer this question.
The COVID-19 crisis provides a unique opportunity to expand the scope of crisis communication research. This paper contributes to crisis and risk communication research, especially to the research on the role of media in a pandemic crisis. Our model showing both the direct effect and the effect mediated by negative feelings of media on preventive behaviors in a pandemic could be further tested in both South Korea and in other societies to better understand how media can directly and indirectly influence willingness to take action to mitigate risk, and may thereby also provide policy makers with insight on how to encourage public health behavior adoption.
Biographical Notes
Sungjoong Kim is a lecturer in the College of Liberal Studies at Chungnam National University. He earned his doctoral degree from Michigan State University, USA and his master’s and bachelor’s degrees from Seoul National University, South Korea. He can be reached at Chungnam National University, College of Liberal Studies 99, Daehak-ro, Yuseong-gu, Daejeon, 305-764, South Korea or by e-mail at sungjoongk@gmail.com.
Sung Kyum Cho is the dean of the Graduate School of Public Policy at Chungnam National University. He was previously the dean of the College of Social Sciences at Chungnam National University. He is the director of the Center for Asian Public Opinion Research and Collaboration Initiative (CAPORCI), where one of the major projects is the KAMOS survey and another is the publication of the Asian Journal for Public Opinion Research (AJPOR). He is a publisher and co-editor of AJPOR. He is also the former president of the Asian Network for Public Opinion Research (ANPOR), the Korean Society for Journalism and Communication Studies, and the Korean Association of Survey Research. He can be reached at Chungnam National University, Department of Communication 99, Daehak-ro, Yuseong-gu, Daejeon 305-764, South Korea or by e-mail at skcho@cnu.ac.kr.
Sarah Prusoff LoCascio is the managing editor of the Asian Journal for Public Opinion Research (AJPOR). She is affiliated with the Center for Asian Public Opinion Research and Collaboration Initiative (CAPORCI). She earned her master’s degree from Indiana University, USA and her bachelor’s degree from Bard College at Simon’s Rock, USA. She can be reached at Chungnam National University, Department of Communication 99, Daehak-ro, Yuseong-gu, Daejeon 305-764, South Korea or by e-mail at sprusoff@alumni.iu.edu.
Correspondence
All correspondence concerning this article should be addressed to Sungjoong Kim at Chungnam National University, College of Liberal Studies 99, Daehak-ro, Yuseong-gu, Daejeon, 305-764, South Korea or by e-mail at sungjoongk@gmail.com.
Date of submission: 2020-07-01
Date of the review results: 2020-08-06
Date of the decision: 2020-08-14