COVID-19 or coronavirus was first identified in Wuhan, China in December 2019 (Zu et al., 2020) and has become an ongoing global pandemic today (Zhou et al., 2020). The virus had reached 114 countries by March 12, 2020, including Indonesia (WHO, 2020). It was confirmed that the virus had infected the Indonesian population on March 2020 (Public Health Emergency Operation Centre, 2020). As of August 14, 2020, the virus had spread to 34 provinces in Indonesia, with a total of 132,816 confirmed cases, 87,558 recovered cases, and 5,968 mortality cases (Public Health Emergency Operation Centre, 2020). Unfortunately, the mortality rate (4.5%) in Indonesia is higher than the rate in Southeast Asia and globally. Thus, efforts to decrease the mortality rate are needed.
Efforts that have been conducted in Indonesia include the large scale social restrictions, stay at or work from home, and social media campaigns with regards to hand washing, physical distancing, and wearing facial masks. However, the progress to decrease the number of COVID-19 cases is relatively slow. It is because some people may not be able to stay at home due to economic problems, and some may be still not understand the truth about COVID-19 cases in Indonesia (Gunawan et al., 2020).
Our study aimed to explore the experiences and attitudes of patients with COVID-19 during the treatment and recovery process. Individual experiences will help others to understand the quality of life issues facing those with COVID-19 in Indonesia of COVID-19. The results of this study are important to inform the community about prevention and to support others during the process. However, the recovery process is dependent on not only the individual but also on the environment and care (Buana, 2020).
Methods
Search Strategy
A search for official reports related to interviews with patient with COVID-19 was conducted on google.com and youtube.com from February to May 2020. We used a secondary data analysis approach, textual/video analysis, as a new and promising way to measure opinions of small subsets of the population in the digital era (Atac et al., 2020). The terms used keywords in English and Indonesian were “patient,” “coronavirus,” “COVID-19,” and “Indonesia.” The official reports on the websites of the world official organizations, Indonesian government agencies, national and international online news, and reliable YouTube channels were included. In this study, we were concerned with reaching a point of understanding patient experiences based on observations in the literature and in video data. Data saturation does not apply to this study, due to this study use of secondary data.
Inclusion Criteria
The inclusion criteria were a video or article of an interview or narration of people with COVID-19 and a patient who has family members with COVID-19.
Screening
The first author did the first screening, and all authors reviewed the included studies and conducted a content analysis together.
Data Analysis
The data were analyzed using latent content analysis (Polit & Beck, 2009) with the following steps. 1) All interviews were transcribed, checked, and re-checked to determine the theme by all researchers. We analyzed the entire text and interpreted it as a whole. 2) We marked meaningful words, phrases, and statements in each transcript. 3) We interpreted the themes of the experience to represent the entire experience and then re-read the transcription to assure that it was appropriate with patient experiences. During analysis, there was no data missing, and the credibility of the data was formed through a discussion among the researchers by comparing and differentiating data quality and interpretation using a method suggested by Gunawan (2015).
Results
Search Outcomes
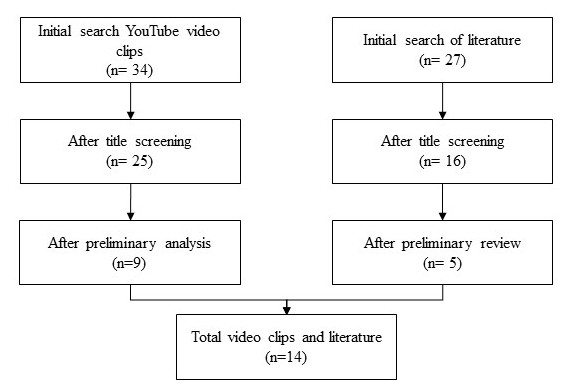
Our initial search identified 34 videos on YouTube and 27 written interviews or narratives. After title screening, 9 videos and 11 articles were removed due to the titles not being related to the topics. Finally, 9 videos and 5 written interviews or narratives were included based on the inclusion criteria, and they were further reviewed (See Figure 1).
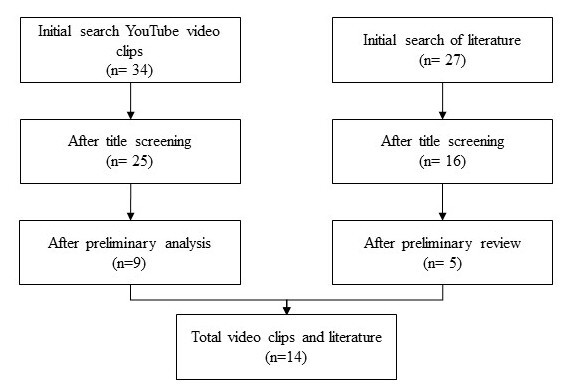
Table 1 shows the results of the data extraction from literature review, with three interview data and two narrations. Table 2 shows the extraction of nine videos from YouTube channels. A total of 13 positive cases and three suspected cases were identified from the data.
Analytical Findings
Five themes were developed in this study:
Theme 1: Experience of Receiving a Diagnosis
There were three subthemes in describing the experience of receiving a diagnosis:
Subtheme 1: I Am Shocked, How Could I Get Infected? Eight patients were surprised when they were first diagnosed with COVID-19 and when they had not been in contact with patients with COVID-19. It is described in the following statements (Patient numbers refer to the numbers assigned in Tables 1 and 2):
“… surprised, I’m shocked. How could I get the virus? How come?” (P4)
“… shocked …” (P2)
Subtheme 2: Suggestive Thinking Between Dead or Alive. Six of the patients, after being diagnosed with COVID-19, thought they were going to die although they had no symptoms. They have been influenced by beliefs from the news about the worst effects of COVID-19. Fear and panic have been described by the patients:
“…after being diagnosed with COVID-19, I started to imagine that I had the symptoms such as cough, cold, fatigue, and sore throat” (p10)
“… My mind thought between life and death because I believed that COVID-19 was between life and death…” (p12)
Subtheme 3: Uncertainty of the Test Result. Seven patients expressed their uncertainty about the results of the COVID-19 test. They needed to wait for almost two weeks to get the results of their test, which posed other problems during the quarantine. It is undeniable that waiting is not an easy task. It was expressed by the participant:
“…I have been waiting for the third result for 12 days. The others [patients] are waiting more than that [12 days]. What is the problem? Thus, I learned that the current condition is our biggest challenge, as the patients need to wait for the result of the swab, which is taking a very long time…” (p2)
Theme 2: Boredom During Isolation
There is no doubt that living in isolation is boring. All of the patients in this study expressed the same feeling during a quarantine for at least 11 days.
P11 expressed, “… Bored bitter!”
P3 said, “…Because in the isolation room we could not meet anyone. The only entertainment was a cellphone, and the only ones who could enter the room were nurses and doctors. It is boring and stressful”.
P9 expressed, “…I need friends to chat with. It is too boring here…”.
Theme 3: Being Stigmatized and Discriminated Against
Eleven patients were stigmatized and discriminated against in the community. They were either confirmed or suspected to have COVID-19. This not only occured among patients but also among their family members. Unfortunately, the community knew the patients’ identities and where they lived, which led to mental health problems for both patients and their family members. However, this situation is also related to the news the community listened to on a daily basis. This is described by the participants:
P7 said, “… I’m surprised why people out there focus only on my identity, not the disease. They reject me and my family in the community…”
P2 expressed, " … it’s a pity that my information leaked on WhatsApp. People know my name, where I live, and what my mobile number is. Even worse, the pressure from the community forms a negative stigma not only for me but also for my family…"
P5 expressed, "… I hope we don’t spread hoaxes that cause fear. I have experienced it. People reported that I was in critical condition when I was taken to the hospital. But actually, I was not. I was driving by myself to the hospital and my car was still in the parking lot … ".
Theme 4: Self-Reflection with God
Eleven patients said that COVID-19 was a test for humans from God. They believe that God will cure them. The participants expressed this:
"…I am kind to God, because if God gave me this disease, so only God can save me. It is just a test… " (p1).
"… I am not a superman and an ordinary human being. I thought about giving up in the face of this big problem, but I still have to fight it. So now what is the way for me to develop a sense of pleasure in my body, in my body, then I have to enjoy, I have to think positive, and pray to God … " (p10).
Theme 5: Social Support from Family Members and Healthcare Workers
Eleven patients revealed that they have support not only from their family but also from the healthcare workers during the treatment for COVID-19. It is described in the following way:
P13 said, "… My family gives me strength for what I am now facing. They keep making video calls to me and ask about me, and they never ask about COVID-19… "
P12 said, " …health workers motivate me also. Every time they always smile and say good morning, Mr. J. I like to make jokes with them. Sincerely, we are fighting together. Also, my family members chat with me every day…"
Discussion
The aim of this study was to explore the experiences of patients with COVID-19 during the treatment and recovery process. We identified five themes as the result of the study, which could be also considered as the stage of the transition process of those with COVID-19.
The theme “experience of receiving a diagnosis” consists of three subthemes, one of which, “I am shocked. How could I get infected?” indicates that many patients did not know how the virus was transmitted among people, with or without the symptoms. Therefore, this response suggests that everyone must be careful and follow the health recommendations completely. In addition, the subtheme “suggestive thinking between dead or alive” has become a concern. The suggestive thinking from what people see on a daily basis about COVID-19 will become their belief. According to the results of this study, there were somatic symptom disorders that made people believe they had transitioned from asymptomatic to symptomatic right after the patients were diagnosed. Somatics symptom disorders were substantially overrepresented among those with mild to serious concerns of the illness (Page et al., 2011). In addition, the subtheme “uncertainty of the test result” indicates that the healthcare system in Indonesia might not be fast enough to deal with the spread of COVID-19. In fact, extra waiting time for the swab test results will exacerbate the patients’ condition, which will lead to a sense of danger and psychological distress (Gunawan et al., 2020).
The theme “boredom during isolation” indicates a serious problem for patients with COVID-19. It is line with a previous study that indicated that the state of isolation or quarantine will lead to loneliness, anxiety, boredom, depression, neglect, stress, and suicide (Gunawan et al., 2020).
The theme “being stigmatized and discriminated against” reflects a continuing serious situation. Although it is understandable that people try to avoid contact with patients and their family members for their own safety, their behaviors can be harmful. Stigmatization and discrimination can be more dangerous than COVID-19 itself, which can lead to suicidal ideation and attempts (Gunawan et al., 2020). As human beings, we are meant to help each other and reduce stigma. In additions to creating stigma, it is recommended that people validate the information they read on the Internet. Based on the data from the Indonesian Ministry of Communications and Informatics, there are over 500 cases of fake news and 101 cases investigated by the police related to COVID-19 (Ministry of Communication and Information, 2020).
Under the theme “self-reflection with God”, COVID-19 may have increased human beings’ awareness of their creator. Although the majority of the patients thought they were at the lowest point of their lives, they believed that God would help them heal. This spiritual value has become an important part of the treatment process, which will provide strength (Juanamasta et al., 2020) as well as happiness, and psychological, social, and emotional well-being benefits (Pawar Badrinarayan, 2016; Pearce et al., 2012; Rowold, 2011) among those with COVID-19.
The last theme, “social support from family members and healthcare workers,” indicated that humans are social creatures who cannot live without social support to deal with illness of COVID-19. Therefore, the family should keep supporting their family members who get infected with the virus, as well as to the healthcare workers to keep their smiles and work with holistic care. A study showed that healthcare practitioners could improve the approach to self-management that helps patients to obtain primary encouragement toward their illnesses (Oftedal et al., 2010). All of the informants got social support via telephone, message, or any kind of social media. Social media expected as future support (Antheunis et al., 2013). Thus this study gives empirical evidence that isolated patients got social support through social media.
This study provided the new insights of the stages of transition process from the first diagnosis until the recovery process following the themes above. We expect that most of the patients might experience all the stages indicated in this study although some stages might be overlapping or emerging in some patients, such as emerged between shocked and suggestive thinking of death or alive, or stigma comes first before boredom. In this study, we also found three patients did not feel shock and fear because they did not experience any symptoms and avoided the suggestive thinking as much as they could. However, this study helps to understand the mental and emotional process of patients during the treatment of COVID-19.
Conclusion
A secondary approach in textual or video analysis was used to gain a more in depth understanding of the attitudes and quality of life of COVID-19 patients than could have been gotten via other methods, for instance surveys. The findings of this study serve as an input for the government, community, and healthcare workers. The study provides basic guidelines to understand the transition process of those with COVID-19. At first, patients should be patient and calm down after they are diagnosed. During isolation and treatment, patients should focus on themselves. Patients should avoid negative thinking, such as stigmatization and discrimination. They could replace this with positive thinking, such as thinking they will get well as soon as possible. Then patients could try self-reflection to control their stress during isolation. To get social support during isolation, patients could contact their close friends or family and talk with the doctor and nurse.
Furthermore, the patients believe that no one could help, except God, family members, and healthcare workers. Therefore, it is suggested for the government to reduce the stigma and discrimination in the community, keep the identity of patients classified, and filter or block any news that spreads panic and fear. For the community, it is suggested they validate information received from the Internet before spreading it. Misinformation may lead to psychosocial disorders. For healthcare workers, it is recommended to always give support, information, and motivation for the benefit of humankind, specifically for those with COVID-19 in the current situation. Further studies related to strategies to reduce stigma and discrimination and the system that supports the rehabilitation and the recovery process of those with COVID-19 are needed.
Biographical Notes
I Gede Juanamasta, BNS, MNS, is a PhD student at the Faculty of Nursing, Chulalongkorn University Bangkok, Thailand and is also affiliated with the nursing program at STIKes Wira Medika Bali, Indonesia. He can be reached at Faculty of Nursing Chulalongkorn University Bangkok Borommaratchachonnani Srisataphat, Building, Rama 1 Road, Pathumwan, Bangkok 10330, Thailand or by e-mail at juana.masta.90@gmail.com.
Yupin Aungsuroch, PhD, RN is an associate professor in the Faculty of Nursing, Chulalongkorn University, Thailand and can be reached at at the Faculty of Nursing, Chulalongkorn University Bangkok, Borommaratchachonnani Srisataphat, Building, Rama 1 Road, Pathumwan, Bangkok 10330, Thailand or by e-mail at yaungsuroch@gmail.com.
Joko Gunawan, BNS, PhD is a postdoctoral researcher, Faculty of Nursing, Chulalongkorn University and can be reached at Faculty of Nursing Chulalongkorn University Bangkok Borommaratchachonnani Srisataphat, Building, Rama 1 Road, Pathumwan, Bangkok 10330 or by e-mail: jokogunawan2015@gmail.com.
Acknowledgement
We acknowledge Chulalongkorn University for the Second Century Fund (C2F).
Correspondence
All correspondence concerning this article can be addressed to Yupin Aungsuroch at the Faculty of Nursing, Chulalongkorn University Bangkok, Borommaratchachonnani Srisataphat, Building, Rama 1 Road, Pathumwan, Bangkok 10330, Thailand or by e-mail at yaungsuroch@gmail.com.
Date of Submission: 2020-06-23
Date of the review results: 2020-08-05
Date of the decision: 2020-08-09