




Background
Chronic Kidney Disease (CKD) is a major cause of illness worldwide, including in Thailand. Currently, among ASEAN countries, Thai people are the 3rd most likely to suffer from chronic kidney disease (Tanakitjaru, 2015). There were about 75,000 patients with end-stage renal disease (ESRD) who received renal replacement therapy (RRT), either hemodialysis (HD) or continuous ambulatory peritoneal dialysis (CAPD) in 2017 (Nephrology Society of Thailand, 2017).
Phraphutthabat Hospital, Saraburi, Thailand is a secondary care hospital that has a kidney unit providing care for ESRD patients who receive either HD or CAPD. Between 2007 and 2015, there were 20-30 ESRD patients receiving dialysis at any time. The number of patients with ESRD receiving dialysis increased after that. In 2016, there were 104 ESRD patients receiving RRT in Phraphutthabat Hospital, according to the medical records maintained by Phraphutthabat Hospital, 2007-2016, which we received authorized permission to access.
Based on the pathological changes related to ESRD, patients have various problems due to kidney degeneration. Increasing poisonous wastes in their body cause dizziness, loss of appetite, weight loss, unconsciousness, blurred vision, diarrhea, loss of feeling in their extremities, itchy, dry skin, and cyanosis. Some feel tired, cry, experience frequent cramping, and/or have irregular heartbeats, chest pain, swelling, ecchymosis, blood in vomit, blood in their stools, anemia, and sleepless (Tanakitjaru et al., 2018). Ukati & Chantajirakhovit (2007) found that the activities of patients with ESRD decreased, and patients also experienced unhappiness, suffering, and hardship in life. There are 2 treatments for chronic renal failure patients: the first is renal transplantation, which is high-cost and requires advanced technology. The patients registered for the transplant waiting list at the tertiary care hospitals. The Universal Coverage Scheme (UCS) covers less than the total cost of treatment for renal transplantation. It requires patients to pay a portion of the expenses themselves. The second is treatment to maintain renal function (HD and CAPD). Phraputtabat Hospital provides only the latter treatments. Patients receive HD directly in Phraphutthabat Hospital around 2-3 times per week for 4-6 hours per session at a high cost for patients covered by UCS. However, the cost of HD is covered without additional payment for those whose healthcare is paid by the Government Officer or Social Security Schemes. In contrast, CAPD exchanges are done by patients at home around 4 times a day, using gravity to help fill their abdomen with dialysate and retain its fluid about 4 hours before draining in 30 minutes. The latter treatment is still economical and requires spending less time at the hospital. Moreover, patients are better able to consume food and water with CAPD compared to HD (Sriyuktasuth et al., 2017).
Quality of life (QOL) means the general well-being of individuals and societies, outlining negative and positive features of life. It observes life satisfaction, including physical health, family, education, employment, wealth, safety, and security to freedom, religious beliefs, and the environment (Post, 2014). QOL differences due to treatment duration and advanced pathology have been reported. RRT may have a significant impact on patients’ perception about various modalities of dialysis. Comparisons of QOL in patients receiving HD or CAPD have produced conflicting results. It is not clear from the previous studies which dialysis method provides better QOL. Then, as nurses, we intend to study the specific area around Phraphutthabat Hospital Saraburi Province, giving particular attention to socio-demographic data. The expected findings should provide more understanding to improve QOL for HD and CAPD patients.
The Phraphutthabat community is situated in a rural area where people often help each other, not only within their own families, but others as well. In addition, this community is ready to support each other using the best services from health promoting hospitals. Health volunteers are able to work closely with the surrounding villages.
Based on our literature review, there are many factors that affect the QOL of chronic renal patients in Thailand including age, marital status, education, occupation, income, type of health coverage, and duration of treatment. Previous studies suggested various factors, for instance age, education, and treatment duration were related to QOL. Age, income, and travel duration were not statistically significant factors in at least one study (Yesonkaw et al., 2016). On the other hand, age was statistically significantly related to QOL in another study (Bunyatnopparat & Anutrakulchai, 2017).
Objectives
1. To compare the QOL of patients with ESRD between patients who receive HD and patients who receive CAPD.
2. To compare the QOL of patients with ESRD with personal characteristic factors such as age, marital status, education level, occupation, family income, type of health coverage, and duration of treatment.
Methodology
Conceptual Framework
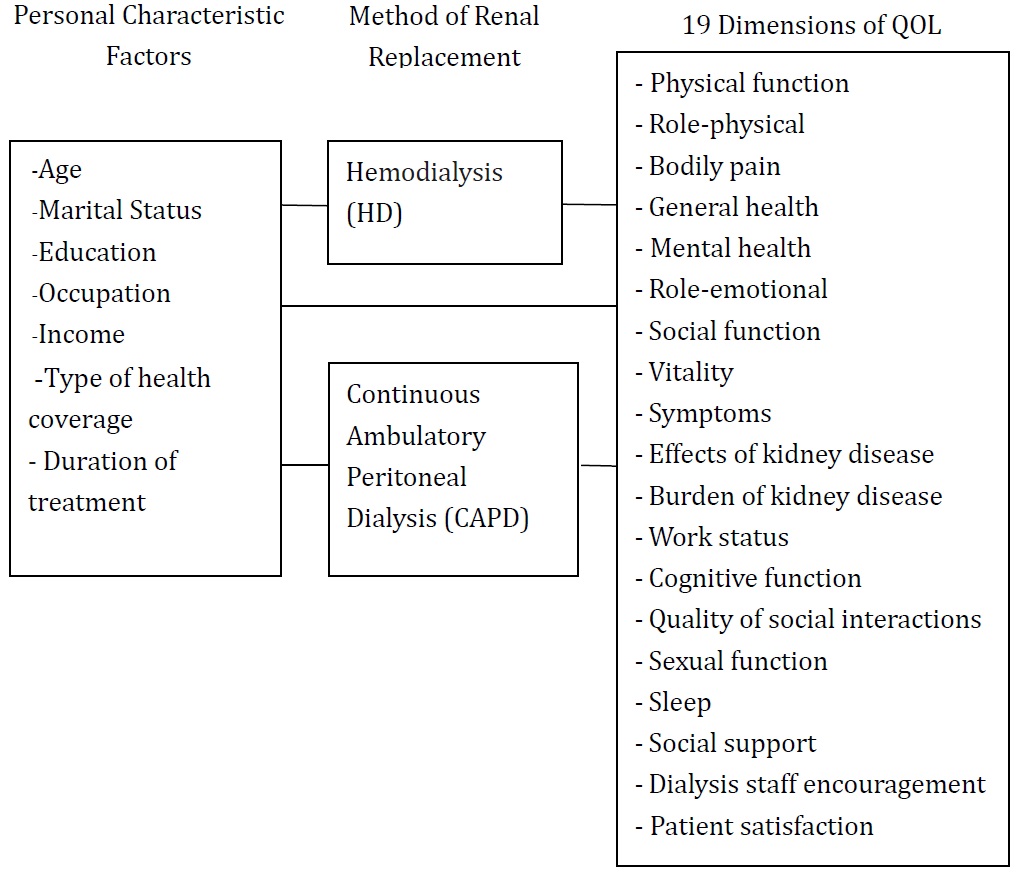
This research aimed to compare the QOL of patients with ESRD who were receiving either HD or CAPD and to compare the QOL of patients with ESRD with different personal characteristic factors. This study was based on the QOL according to the Kidney Disease Quality of Life Working Group in the United States. This concept was presented as part of holistic care, including physical, mental, and social aspects, which can consequently prolong life and decrease mortality. This major concept of QOL was divided into 19 dimensions. The conceptual framework for the research is as follows.

Population and Sample
The population is patients with ESRD who were receiving either HD (48 persons) or CAPD (57 persons) at Phraphutthabat Hospital during the 2015-2016 fiscal year. The total population includes 105 persons. Of these, 76 patients were selected, of whom 39 received HD and the remainder (37 patients) received CAPD. The inclusion criteria were 1) no communication problems, 2) normal awareness and consciousness, 3) born in Saraburi province 4) routine follow up in Phraphutthabat Hospital 5) Patients consciously and voluntarily agreed to participate in the research.
Research Instrument
The KDQOL-SFTM Version 1.3 was created by the Kidney Disease Quality of Life-Working Group USA. It was revised and translated into Thai with input from experts. The process of instrument development was a cognitive interview and concurrent probing interview of 15 renal dialysis patients. All items’ meaning in Thai were informative based on psychometric properties. The study was conducted in 2009. The research group was 191 patients receiving dialysis therapy due to chronic renal failure. Coefficient alphas ranged from .44 to .86. The coefficient of item-total correlation ranged from .53 to .95. The convergent validity was 74.17%. The discriminative validity was 88.81%. For this study, Cronbach’s alpha was .73. The KDQOL-SFTM Version 1.3 is an 80-item instrument consisting of 19 dimensions measured using a 5-point Likert scale. The detailed scoring instructions for this instrument (Hays et al., 1995) result in a score 0-100, which can be used to divide overall quality of life into five categories: the lowest (<50 points), low (50-59 points), moderate (60 - 69 points), high (70-79 points), and the highest (>=80 points) (Homjean, 2009). The KDQOL-SFTM Version 1.3 is composed of nineteen dimensions of QOL, including physical function, (12 items), role-physical (4 items), bodily pain (2 items), general health (5 items), mental health (5 items), role-emotional (3 items), social function (2 items), vitality (4 items), symptoms (12 items), effects of kidney disease (8 items), burden of kidney disease (4 items), work status (2 items), cognitive function (3 items), quality of social interaction (3 items), sexual function (2 items), sleep (4 items), social support (2 items), dialysis staff encouragement (2 items), and patient satisfaction (1 item).
Data Collection
Data were collected from April to September 2016. This research was approved by the Ethics Committee on Human Research of Boromarajonani Nursing College Phraphutthabat. The Certificate number was EC002/2016. The patients completed survey by 30-40 minutes at renal unit. All literate patients responded themselves but researchers or team members read the questionnaire to respondents who could not read.
Data Analysis
Socio-demographic data and QOL were analysed by frequencies, percentages, means, and standard deviations. The comparison of QOL scores between patients who received HD and CAPD was conducted using independent t-tests. The comparisons between QOL and socio-demographic data used independent t-tests and ANOVA.
Results
Socio-Demographic Data
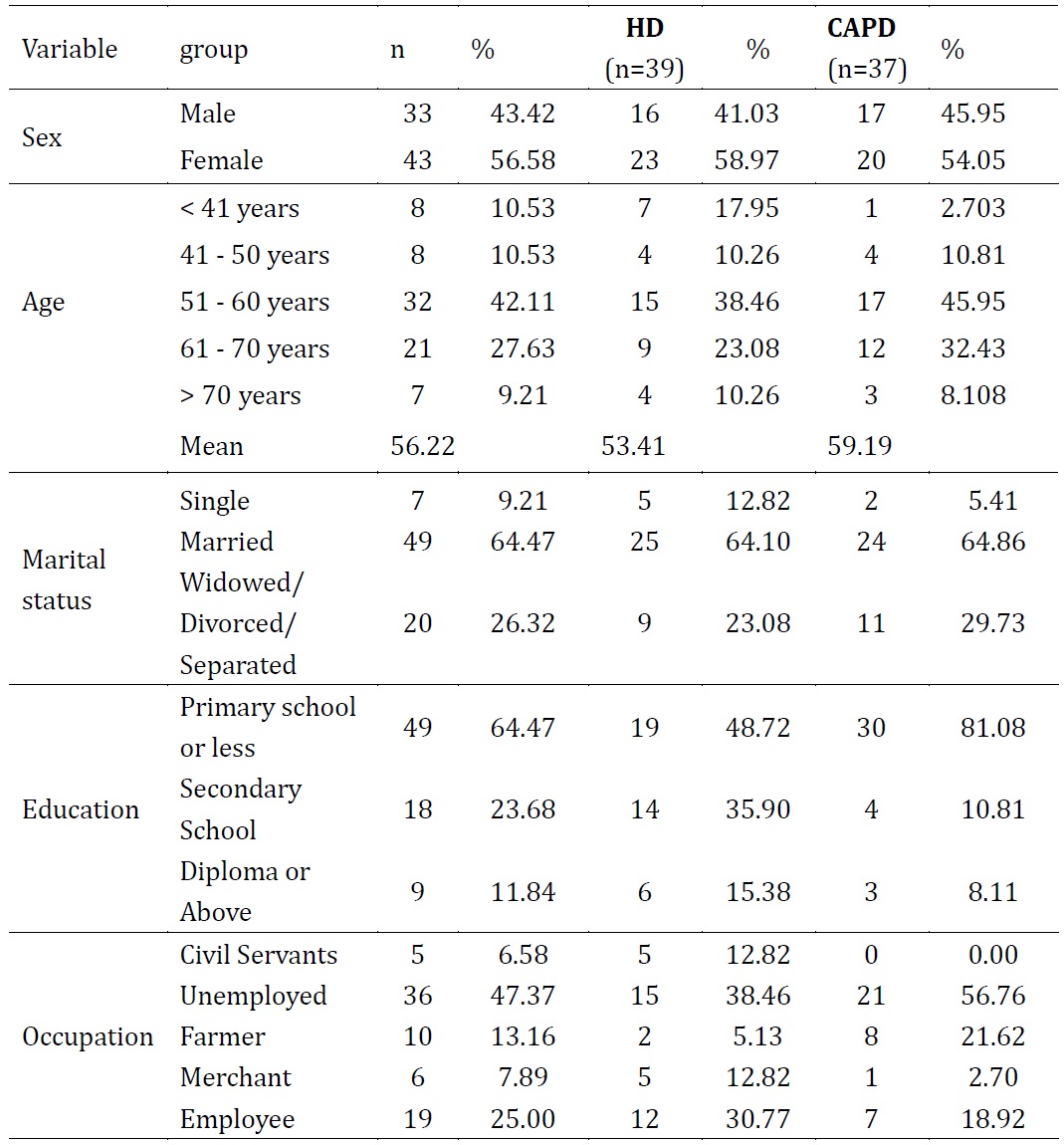
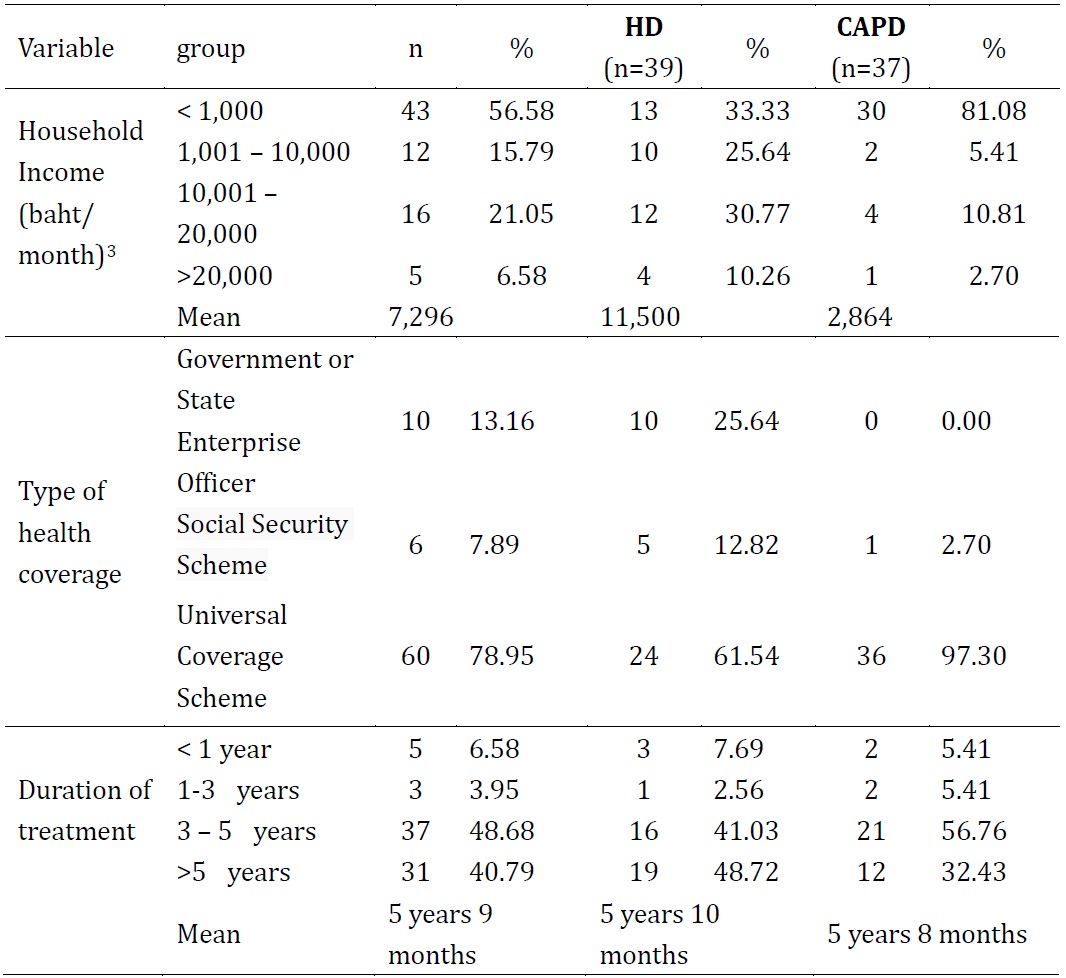
The majority of HD (58.97%) and CAPD (54.05%) patients are female. The mean age was 53 years old for HD patients and 59 years old for CAPD patients. Most of them were married (64.10% of HD; 64.86% of CAPD). The majority had attained an education level of no higher than primary school (48.72% of HD; 81.08% of CAPD). The majority were unemployed (38.46% of HD, 56.76% of CAPD). The mean family income was 11,500 baht/month (approximately $361US) for patients receiving HD and 2,864.86 baht/month (approximately $90US) for patients receiving CAPD. The majority received healthcare under the UCS (61.54% of HD; 97.30% of CAPD). The mean duration of treatment was 5 years, 10 months (HD) and 5 years, 8 months (CAPD).
The socio-demographic data of HD and CAPD patients is shown in Table 1.


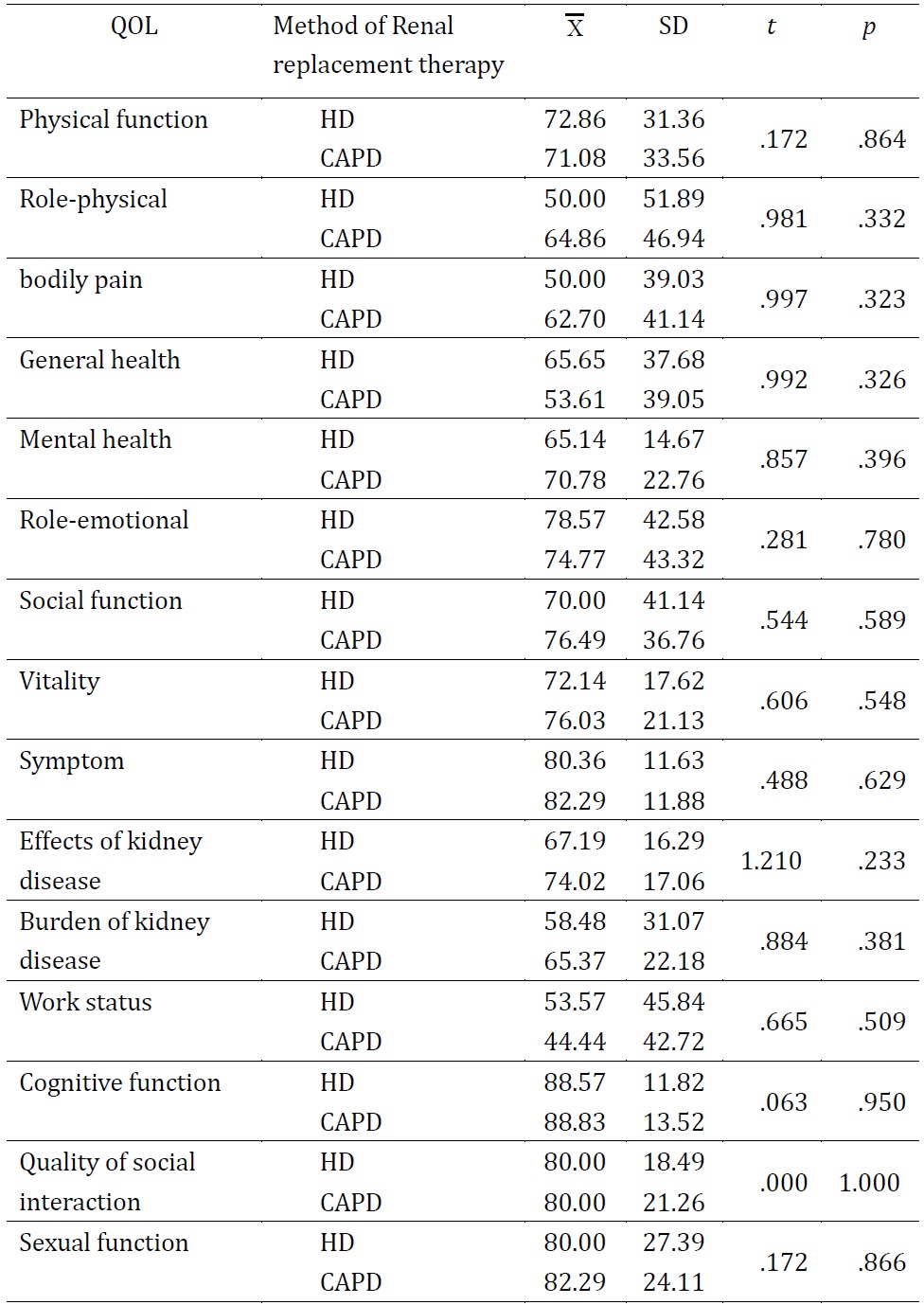
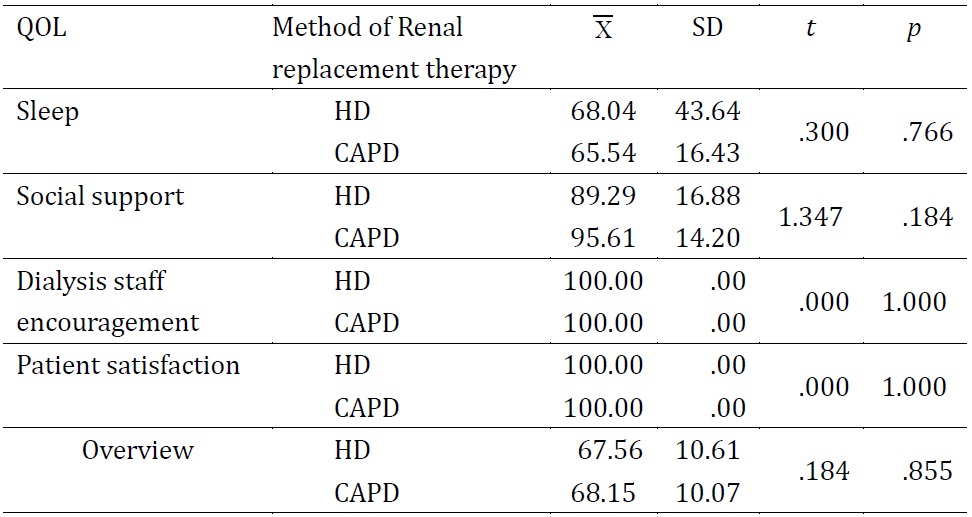
Overall, patients receiving HD or CAPD had a moderate QOL (X=67.56, SD=10.61 and X=68.15, SD=10.07, respectively). The QOL of patients receiving HD and CAPD is shown in Table 2.

The highest dimension of QOL was dialysis staff encouragement and patient satisfaction =100, SD =0.00) in both groups. For QOL of patients receiving HD, the dimensions with the lowest scores were role-physical =50.00, SD=51.89) and bodily pain =50.00, SD=39.03), respectively. For patients receiving CAPD, the lowest score was work status =44.44, SD=42.72).


The results (see Table 3) showed that patients receiving HD had a higher the QOL than the CAPD group in terms of the following 5 dimensions: physical function, general health, role-emotional, work status, and sleep. There was no difference between patients in the two treatment groups in the following QOL dimensions: quality of social interaction, dialysis staff encouragement, and patient satisfaction. The differences in the other dimensions of QOL were not statistically significant.
Comparison of the QOL and Socio-Demographic Factors
A comparison of the QOL of patients receiving RRT with socio-demographic factors are presented in Tables 4 and 5.

The QOL of male and female patients was not different.

Table 5 shows that the QOL of patients receiving RRT for ESRD was not related to their age, marital status, education, occupation, or type of health coverage. Their QOL was related (for at least one pair) to their income level (p=.008) and duration of treatment (p<.001).

Table 6 shows that the difference in QOL of patients with ESRD between those with almost no income (<1,000 baht/month or $34US) and all other income groups was different at least the .05 level (p=.008-.041). There was no statistically significant difference among the other income groups.

ESRD patients who have been receiving treatment for more than 5 years have a significantly higher QOL at least the .05 level.
Discussion
Patients receiving HD and CAPD had a moderate overall QOL because both methods were time consuming. Treatment affected their work and social life, and they also had expenses for some equipment of HD treatment and also traveling to the hospital. In addition, the cost of treatment increased. They depended on caregivers to take them to the hospital. They experienced poor health, low immune function, and it was easy for them to get infections. It is difficult to live a normal life, and so they faced a reduced quality of life. However, caregivers and nurses took good care of them. There were three dimensions that showed a high mean score including 1) dialysis staff encouragement, 2) social support and 3) patient satisfaction. However, the overall mean score QOL was moderate. The findings support results of previous studies. Aiyasanon (2009) and Ukati & Chantajirakhovit (2007) studied RRT by HD and CAPD. The results of these studies revealed a moderate QOL in both groups.
Based on the comparison between permanent HD and CAPD patients, there was no statistical difference in QOL overall or in any specific dimension. This might be caused by other specific support, for instance support from relatives and health staff. Respondents reside in a rural area with help from extended family members and health staff in the hemodialysis unit. As a result, satisfaction with the health staff and treatment had the highest possible score =100, SD.=0.00). Respondents were ready and confident to address their health problems. There were no statistical differences in QOL compared to patients receiving HD or CAPD in Northern, Thailand (Laolam et al., 2014).
ESRD patients did not experience a statistically different QOL based on age, marital status, educational level, occupation, or type of health coverage. However, QOL was related to income and duration of treatment. Patients with low incomes had a lower QOL than those who had higher incomes. Therefore, income is a significant factor affecting QOL, which is consistent with Russo et al. (2010) and Wichaisak (2017). Moreover, other studies (Khomwong et al., 2011; Wanachad et al., 2015) have also found a statistically significant connection between income and QOL. In addition, patients who had spent much time in chemotherapy had a higher QOL than those who had been in treatment for less time. Knowledge, understanding of self-management, and health acceptance are factors that support better patient living adaptations. These findings supported QOL being positively related to the factors family income and a treatment duration of at least four years (Wichaisak, 2017).
Recommendations
Suggestions for Applying the Research Results in Other Patients
The results of the study show that patients being treated with CAPD had the lowest QOL in work status. To improve the QOL of patients, intermittent peritoneal dialysis or automated peritoneal dialysis that provides dialysis continuing at night could be used. This would contribute to allowing patients to work regularly during the day. We recommend that the government should allow the patients to rent the automated peritoneal dialysis machine at a lower cost. HD patients had a limited QOL due to physical problems and pain. Therefore, physicians and health care staff should be aware of the patients’ problems by understanding methods to control electrolytes, blood urea nitrogen, and creatinine during each dialysis treatment.
Suggestions for Future Research
Researchers should continue to study the QOL of individual patients with renal failure who presented low scores in various dimensions and study the predictive factors of QOL of patients with renal failure who receive RRT treatment.
Biographical Notes
Soontaree Sittisongkram is a nursing instructor, senior professional level at Boromarajonani College of Nursing Phraphutthabat. She completed her Master of Nursing Science (M.N.S.) at the Faculty of Nursing Chulalongkorn University, Bangkok, Thailand.
She can be reached at Boromarajonani College of Nursing, Phraphutthabat, 91 Moo 8 Thankasam, Phraputthabat District, Saraburi, Thailand, 18120 or by e-mail at soontare.s@bcnpb.ac.th.
Jamras Sarakwan is a nursing instructor, senior professional level at Boromarajonani College of Nursing Phraphutthabat. She completed her Master of Nursing Science (M.N.S.) at the Faculty of Nursing at Mahidol University, Bangkok, Thailand.
She can be reached at Boromarajonani College of Nursing, Phraphutthabat, 91 Moo 8 Thankasam, Phraputthabat District, Saraburi, Thailand, 18120 or by e-mail at Jumras1964@yahoo.com.
Phakatip Poysungnoen is a nursing instructor, professional level at Boromarajonani College of Nursing Phraphutthabat. She completed her Master of Nursing Science (M.N.S.) at the Faculty of Nursing at Khon Kaen University, Khon Kaen Province, Thailand.
She can be reached at Boromarajonani College of Nursing, Phraphutthabat, 91 Moo 8 Thankasam, Phraputtabat, Saraburi, Thailand, 18120 or by e-mail at Phaka_poy@yahoo.com.
Malee Meepaen is a registered nurse, professional level at the renal clinic, Phraphutthabat Hospital, Saraburi, Thailand. She completed her Bachelor of Nursing Science (B.N.S.) at Boromarajonani College of Nursing, Saraburi, Saraburi, Thailand.
She can be reached at Phraphutthabat Hospital, 86 Moo 8 Thankasam, Phraputthabat District, Saraburi, Thailand, 18120 or by e-mail at p_renal@pbh.go.th.
Funding Note
This research was supported by the Boromarajonani College of Nursing Praphutthabat, Saraburi, Thailand.
Date of submission: 2018-11-09
Date of the review result: 2019-04-07
Date of the decision: 2019-05-12